Exploration of RBE optimization in proton arc therapy
PO-1726
Abstract
Exploration of RBE optimization in proton arc therapy
Authors: Helge Henjum1, Sara Pilskog1,2, Camilla H. Stokkevåg3,2, Johannes Tjelta3,2, Kristian S. Ytre-Hauge1
1University of Bergen, Institute of Physics and Technology, Bergen, Norway; 2Haukeland University Hospital, Department of Oncology and Medical Physics, Bergen, Norway; 3University of Bergen, Institute for Physics and Technology, Bergen, Norway
Show Affiliations
Hide Affiliations
Purpose or Objective
In clinical proton therapy a
relative biological effectiveness (RBE) of 1.1 is used, although it is known
that the RBE varies and depends on several factors as the LET, tissue type and
dose. This has given rise to several different variable RBE models which aim to
give a more accurate description of the effects of protons. Proton arc therapy
(PAT) is an emerging treatment modality and has showed promise in improving
both target coverage and reducing linear energy transfer (LET) in organs at
risk (OARs). In the current study we further investigate the potential of RBE
based optimization in PAT, employing both full and pruned arc configurations in
treatment of complex tumours surrounding critical OARs.
Material and Methods
Intensity modulated proton therapy
(IMPT) and PAT plans for a paediatric ependymoma patient were created. The PAT plans consisted of a 240° arc, where
the front of the patient received no fields (Figure 1a). Additionally, the
pencil beam spots in the arc plan (denoted full PAT plan) with the highest
energies in each direction were removed to create a pruned PAT plan (Figure 1b
and c), to see if the LET could be elevated in the target while still
maintaining the same tumour coverage. The plans were optimized using a FLUKA Monte
Carlo based optimization tool with respect to two different variable RBE
models, the McNamara model (MCN), and an LET-weighted dose model (LWD), and additionally
an RBE of 1.1. As the tumour was surrounding the brainstem, sparing this
critical OAR had high priority during optimization. The PAT plans were compared to a reference IMPT plan in terms
of their respective RBE weighted doses, physical dose and dose averaged LET
(LETd). 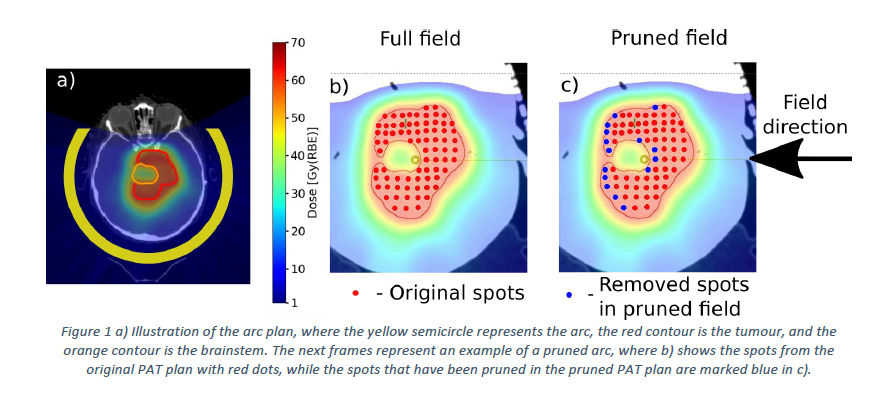
Results
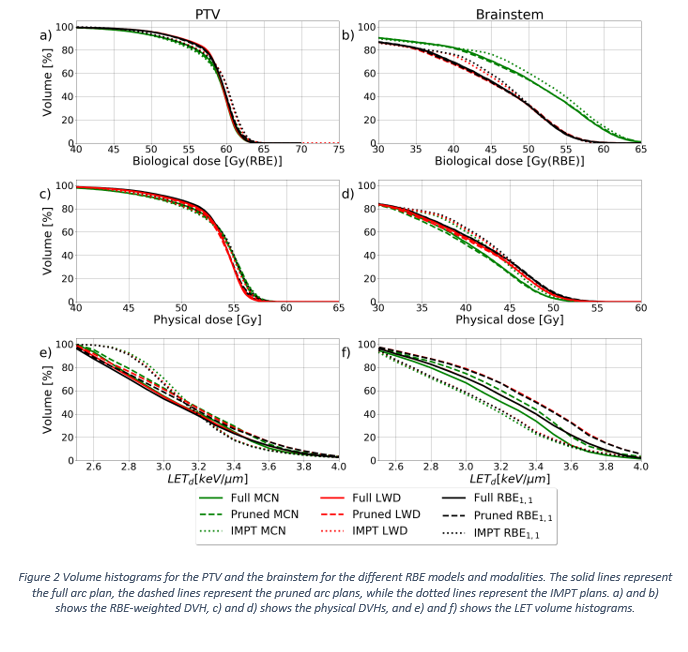
Tumour coverage was
achieved for all plans in terms of (respective) RBE-weighted dose (Figure 1a). PAT
resulted in lower mean physical doses in the brainstem by up to 0.9 Gy and 1.2
Gy for the full PAT plans and the pruned PAT plans compared to IMPT (Figure 2d),
respectively, while there was an increase in LETd in the brainstem for the PAT
plans compared to the IMPT (Figure 2f). This could be expected as the brainstem
is located in the middle of the target. However, the RBE-weighted dose was lower
for the PAT plans in general, compared to the IMPT plan. We
also found the MCN plans providing an overall lower LETd to the brainstem
compared to the LWD and the RBE1.1 plans (Figure 2f).
Conclusion
In this study we demonstrated methods for optimizing PAT plans with
respect to variable RBE models, and the potential of using PAT plans in
treatment planning, both with full arcs and pruned arcs. Although there was an
increase of LET in the brainstem for the PAT plans, the physical doses and the
RBE weighted doses were lower in the brainstem compared to the IMPT plan.