Clinical evaluation of a novel system for real time monitoring of deep inspiration breath hold
Martijn Kusters,
The Netherlands
PO-1679
Abstract
Clinical evaluation of a novel system for real time monitoring of deep inspiration breath hold
Authors: Martijn Kusters1, Emmy van Bronkhorst-van denBos1, Liesbeth Bieamans-VanKastel1, Paulien Westhoff1, Hanneke Meijer1, Jaco Barnhoorn2, Mark Luesink2
1Radboud university medical center, Radiation Oncology, Nijmegen, The Netherlands; 2Cablon Medical, Radiation Oncology, Leusden, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
It is recommended that left breast radiotherapy is performed with deep inspiration breath hold (DIBH), since this results in a significant reduction in radiation dose to the heart and left anterior descending coronary artery.
In this study a newly developed system for real-time monitoring of DIBHs has been tested and evaluated during treatment of 27 patients during breast cancer radiation treatment.
Material and Methods
Patients with left sided breast cancer are guided to perform a voluntary breath hold using verbal instructions and a device touching the abdomen providing sensible feedback. The number of breath holds that are necessary depends on the delivery technique and can vary between 4 and 10.
The system “CNERGY Breath Hold” (Cablon Medical, Leusden, The Netherlands) consists of a single full HD real-time depth camera, installed at the ceiling of the treatment room that measures the respiratory motion of the chest by tracking the surrounding area of the fixed marked tattoo point on the patient’s xiphoid process. During setup this tattoo point is aligned in DIBH at the isocentre of the linac (Elekta, Crawley, UK), where the baseline of the DIBH is defined as 0 mm. When the couch is moved for treatment this translation is also translated in the monitoring system to keep track at the same point on the patient.
The system allows RTTs in the control room to monitor the breath holds during treatment. The system will interrupt the treatment automatically when the DIBHs are not performed well and are outside the gating window of -5 to 5 mm.
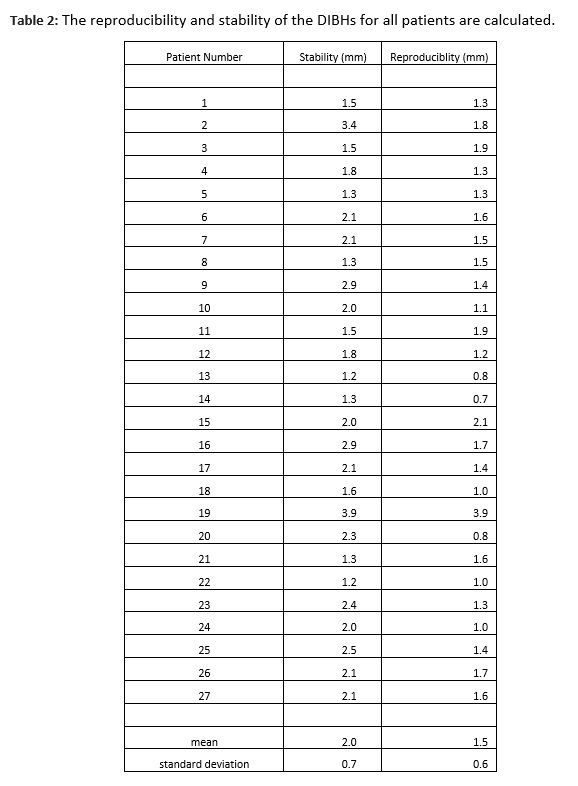
The DIBH data was analysed for reproducibility and stability. For reproducibility the standard deviation of the mean of each DIBH level was calculated. For stability all breath holds were fitted by first order polynomials, the slopes were multiplied by their breath hold lengths to find a range and all these ranges were averaged.
Results
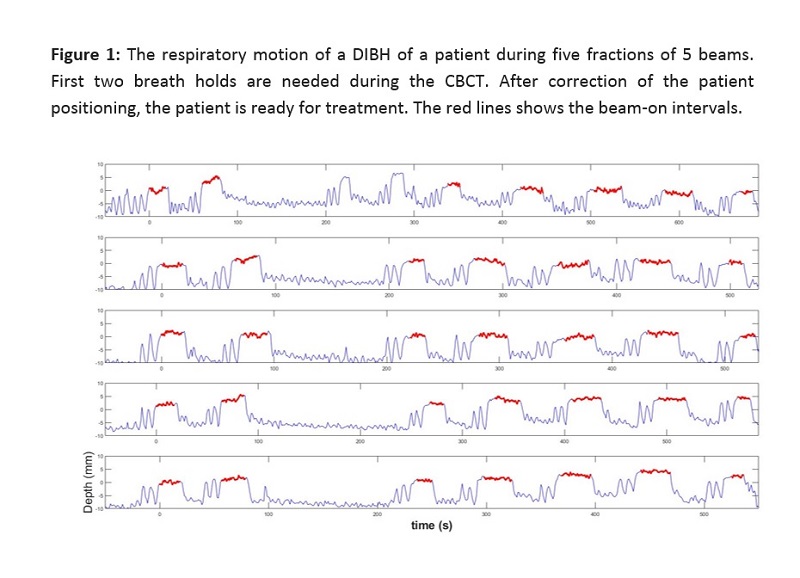
27 patient were treated whereby the monitoring system was active and the respiratory motion during all fractions were monitored and logged. Figure 1 shows the respiratory motion during treatment of a patient for 5 different fractions. First two DIBHS are used for CBCT. Patient position is then checked and corrected. Then 5 beams are treated in DIBHs.
The reproducibility and stability of the DIBHs for all patients are shown in Table 1. The mean stability and reproducibility for all 27 patients were 1.9 mm (SD 0.7mm ) and 1.4 mm (SD 0.6 mm), respectively.
In the current system there is a delay of 3-5 seconds before the radiation will start after the breath hold command is given, which is partially due to the preparation state of Elekta linac. The noise in the measured signal of the system was about 1 mm.
Conclusion
The system detects when the DIBH is not within the gating window. The position of the chest wall is accurately monitored during the treatment and changes in chest wall position during treatment can be easily detected.