Feasibility of robotic stereotactic body radiation therapy for palliative bile duct obstruction .
PO-1675
Abstract
Feasibility of robotic stereotactic body radiation therapy for palliative bile duct obstruction .
Authors: Jan Seppälä1, Jan-Erik Palmgren1, Ananta Pandey2
1Kuopio University Hospital, Radiotherapy Department, Kuopio, Finland; 2University of Easter Finland, Department of Applied Physics, Kuopio, Finland
Show Affiliations
Hide Affiliations
Purpose or Objective
It has been
shown that high dose intraluminal high dose rate brachytherapy (BT) is superior
to stent alone in terms of stent occlusion and mean survival in the palliative
treatment of malignant bile duct obstruction [1, 2]. The most common
complication associated with BT treatment has been duodenal ulceration, which
could, in addition to high doses delivered, result from highly non-uniform dose
distributions of BT treatments [2]. In this study, we evaluated the feasibility
of CyberKnife (CK) radiosurgery system to deliver a single high dose to the
stented area, allowing more flexibility in achieving high dose coverage and
delivering accurate dose distribution in various treatment anatomies.
Material and Methods
3D
printed phantoms along with dynamic motion CIRS phantom capable of resembling
breathing motion were used for irradiating treatment plans created with
Multiplan TPS and Oncentra Brachy TPS. Three different treatment geometries were
simulated: A) straight, B) curved and C) branched stent (Fig 1). Four fiducial
markers were attached around the metallic stents and the stents were inserted
inside the phantoms. EBT3 radiochromic films were inserted in the middle of the
split stents to measure the delivered 2D dose distributions. A 15 Gy single
fraction dose irradiations were performed in static and moving conditions with
the CK system and with the aid of Synchrony Respiratory Tracking System. With
BT treatments, only a static phantom was used. All the irradiations were
repeated twice and two films were irradiated simultaneously, thus four films in
total for each scenario were irradiated and analysed.
Results
The global gamma
index (±3mm / ±3%) was used to compare the
agreement between measured and calculated 2D-dose distributions. The results
are presented in Table 1. Overall, the agreement with CK irradiations was around 95%, with the exception of
branched stationary phantom (84.3%). With BT the gamma agreement was also close to 95% with straight and branched geometries,
but with the curved geometry the agreement was only 68.4%. This might be due
the snaking effect of the source wire or catheter positioning inside the stent.
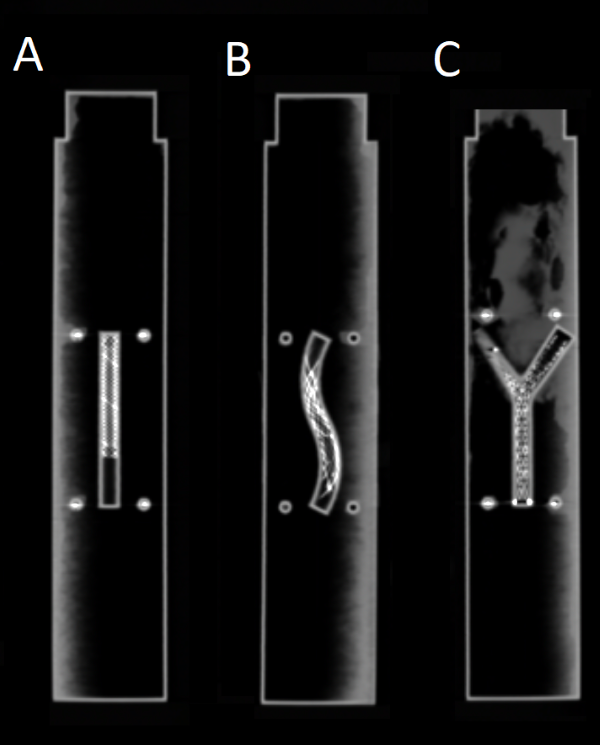
Figure
1: Three different stent geometries: A) straight, B), curved and C) branched
stent.
Table
1: Global gamma index (±3mm / ±3%) of the three geometries for the calculated
and measured CyberKnife and Brachytherapy treatments.
| CyberKnife |
|
|
| Brachytherapy |
|
| Stationary
phantom |
| Moving
phantom |
| Stationary
phantom |
|
| Pass
% | Average | Pass
% | Average | Pass
% | Average |
| Straight | 97.7 | 0.37 | 96.3 | 0.37
| 96.1
| 0.33
|
| Curved | 96.1
| 0.42
| 94.9
| 0.44
| 68.4
| 0.79
|
| Branched | 84.3
| 0.60
| 93.1
| 0.44
| 93.8
| 0.42
|
Conclusion
The
CK system was able to track and treat the moving 3D phantoms resembling bile
duct obstruction after stent placement using fiducial markers. CK was able to
produce accurate dose distributions in the moving phantom and could be an
option for the palliative treatment of bile duct obstruction. The dose delivery
accuracy was also comparable to BT.