Going from planar kV-MV to kV-kV setup images in image-guided radiotherapy of breast cancer
Susanne Nørring Bekke,
Denmark
PO-1674
Abstract
Going from planar kV-MV to kV-kV setup images in image-guided radiotherapy of breast cancer
Authors: Susanne Nørring Bekke1, K Andersen1, CP Behrens1, D Sjöström1, P Sibolt1, SMS Damkjær1
1Copenhagen University Hospital – Herlev and Gentofte, Dept of Oncology, Copenhagen, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
In routine IGRT of patients
with breast cancer, positioning is often based on a tangential MV and an
orthogonal kV image (kV-MV setup) prior to treatment delivery. It is convincing
to see the target (breast) in the beams-eye view with the MV image, but it can
be challenging to interpret setup difficulties in the form of e.g. rotations or
arm position based on a kV-MV setup. In the present study a setup based on an anterior-posterior
(AP) kV image and a lateral kV image (kV-kV setup) is evaluated using MV images
acquired during treatment delivery for
patients treated in Free-Breathing (FB) or Deep Inspiration Breath-Hold (DIBH).
In addition, the yaw rotation setup error is quantified.
Material and Methods
The analysis
was based on 84 fractions from 11 patients treated with 3D conformal
radiotherapy with tangential fields after breast conserving surgery, with and
without lymph node involvement. The DIBH technique was used for 7 patients. To evaluate
the setup deviations in the AP direction (vertical) between the kV-kV setup and
MV images, MV images were acquired during treatment delivery for the two open
tangential fields (n = 168). The setup deviations between the two unpaired
groups treated with FB or DIBH was compared using a Wilcoxon rank sum test. Furthermore,
the yaw setup correction from the initial patient position, based on in-room
lasers and tatoo marks, were retrospecitvly collected based on the kV-kV setup.
Yaw setup corrections above 3 degrees requires repositioning in the clinical
setting in our institution.
Results
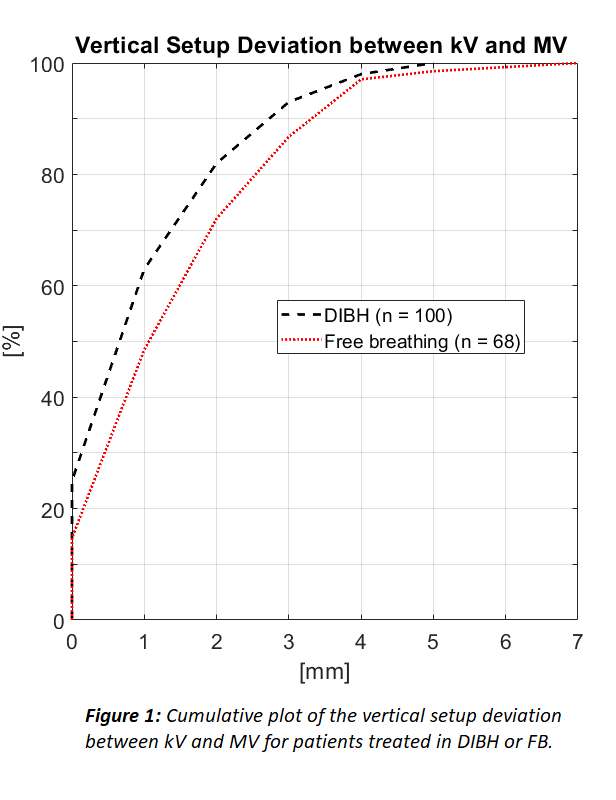
Absolute vertical setup deviations
were ≤ 4 mm in 98 % and 97 % of the acquired MV images in DIBH and FB
respectively (Figure 1). The setup deviations was found to be statistically significantly
larger (p = 0.01) for patients treated in FB (median 2 mm) compared to DIBH (median
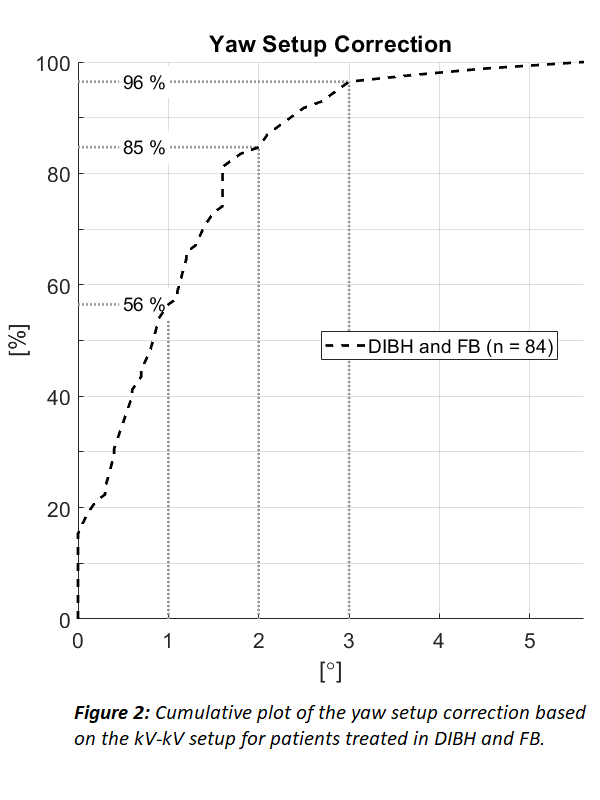
1 mm). The patient position correction based on the kV-kV setup led to yaw
setup corrections within 1° and 2° in 56 % and 85 % of the treatment fractions,
respectively (Figure 2). In 4 % of the treatment fractions the yaw setup corrections
was above 3°, which would require patient repositioning.
Conclusion
Setup
of breast cancer patients based on planar kV-kV images was observed to be in
good agreement with tangential MV images in both FB and DIBH. The setup deviation was statistical significantly larger for patients treated with FB
compared to DIBH, however the difference in median was small (1 mm). With a
kV-kV based setup it is possible to correct for yaw rotations, which based on
the present study was above 2° in 15 % of the treatment fractions. Other
advanatages using kV-kV for breast setup are visualization of surgical clips
and heart.