Correction of target shape changes in bladder cancer patients using online adaptive radiotherapy
Lisanne Zwart,
The Netherlands
PO-1673
Abstract
Correction of target shape changes in bladder cancer patients using online adaptive radiotherapy
Authors: Lisanne Zwart1, Liselotte ten Asbroek1, Erik van Dieren1, Judith Dasselaar1, Francisca Ong1
1Medisch Spectrum Twente, Radiotherapy, Enschede, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
In current clinical practice CTV-PTV margins of 1.5-2.0 cm are used for
image-guided radiotherapy (IGRT) for bladder cancer patients to compensate for
inter-fractional variations of bladder filling. This relatively large margin
results in a substantial dose to the surrounding organs at risk (OARs). CBCT-guided
online adaptive radiotherapy (oART) can be used to correct for inter-fractional
bladder filling variations, resulting ultimately in a treatment with smaller
CTV-PTV margins. The aim of this study was to analyze the value of oART for
bladder cancer patients in terms of target coverage and bladder filling
variations.
Material and Methods
Between July and October 2021, three bladder cancer patients were
clinically treated with CBCT-guided oART using Ethos therapy (Varian Medical
Systems, Palo Alto, CA, US). Two patients were treated with radiotherapy alone
using a fractionation scheme of 20×2.75 Gy. One patient was treated with chemoradiotherapy using a
fractionation scheme of 33×2 Gy. For all
patients a reference 9- or 12-field IMRT plan was created on an empty bladder
planning CT, applying a CTV-PTV margin of 5 mm in lateral and 8 mm in
superior-inferior and anterior-posterior direction. During the adaptive
workflow on couch, two treatment plans were created based on the OAR and CTV
contours on the CBCT. The scheduled plan is the recalculated reference plan and
the adapted plan is the re-optimized reference plan on the daily CBCT anatomy. Both
plans were compared based on coverage of the PTV (V95%≥99%). Moreover, volume
differences of the PTV on the daily CBCT relative to the planning CT were
analyzed.
Results
Volume differences of the PTV on the daily CBCT relative to the planning
CT and dose differences between adapted and scheduled plans are plotted in
Figure 1. The volume of the PTV on the daily CBCT was smaller compared to the
planning CT in 51/73 fractions (69.9%). Even so, the adapted plan was chosen in
all fractions because of increased coverage of the PTV (V95%) with respect to
the scheduled plan. The adapted plan showed a coverage of ≥99% in all cases,
whereas for the scheduled plan this was only in 2/73 cases, with a mean
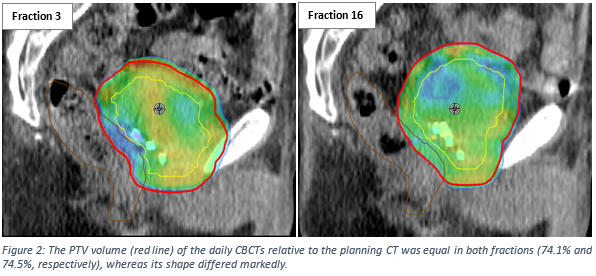
coverage of 94.6%±3.3% (range 84.3% – 99.1%). Figure 2 shows the CBCTs of two
separate fractions in which the volume of both PTVs were comparable, whereas
the shape of the PTVs was completely different.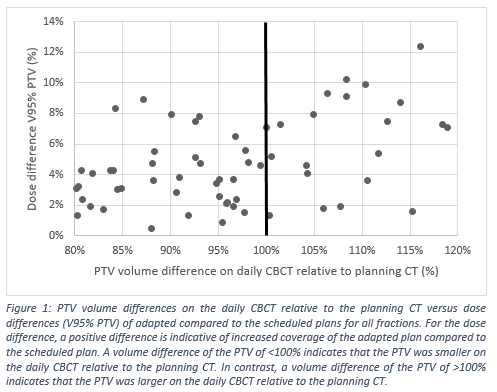
Conclusion
Target coverage was superior in the adapted plans as compared to the
scheduled plans, even in cases with decreased target volume when the scheduled
plan would be deemed sufficient. Therefore shape changes of the target volume play
an important role, which cannot be corrected for using an IGRT or plan of the
day approach. Further analysis with more patients is ongoing.