Back arching during tangential DIBH breast RT detected with live EPID based position monitoring
PO-1654
Abstract
Back arching during tangential DIBH breast RT detected with live EPID based position monitoring
Authors: Elena Vasina1, Natalie Kong2, Jane Ludbrook2, Geetha Govindarajulu2, Peter Greer2, Joerg Lehmann2
1University of Newcastle, NSW, Australia, School of Information and Physical Sciences, Callaghan, Australia; 2Calvary Mater Newcastle, Radiation Oncology Department, Waratah, Australia
Show Affiliations
Hide Affiliations
Purpose or Objective
An electronic portal image device (EPID) based system for real-time monitoring of
breath-hold quality during deep inspiration breath-hold (DIBH) breast cancer
treatments has been developed [1]. Live EPID-based Inspiration Level Assessment
(LEILA) uses internal surrogates, the position of the bony chest wall and the
patient’s skin, to assess the alignment of anatomy with the treatment beam.
LEILA is currently being tested with patients. Its ability to measure at
multiple locations has been utilized to identify instances where the patient
arched their back instead of taking a deep breath-hold, which is known cause of
lower DIBH quality. [2]
Material and Methods
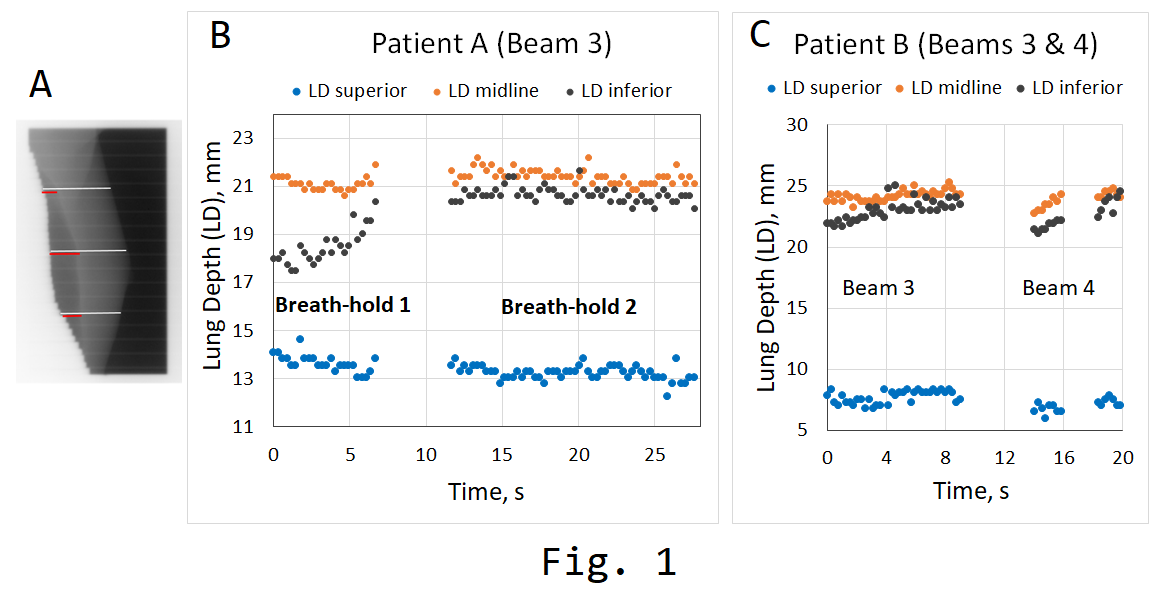
LEILA
analyses portal MV images of breast tangents and measures the lung depth (LD)
and the distance from the skin to posterior field edge (skin distance, SD) at 3
user-selected locations as shown in Figure 1A. It displays these six parameters
in real time and tracks them over time. In this study, breathing and
breath-hold of the patients during RT were monitored and directed with the
Varian’s RPM or C-RAD’s Catalyst+ systems. In both situations, the breathing
window, the allowed motion, was 5 mm.
Results
The
plots of LDs during “Breath-hold 2” in Figure 1B show typical time traces of the
3 LD parameters (superior, midline, and inferior) seen during the DIBH treatments:
the time dependences of the superior, midline, and inferior LDs are changing in
the same direction. For two patients on the study (Patient A and Patient B)
there were instances when the superior LD was decreasing while the midline and inferior
LDs were increasing (“Breath-hold 1” in Fig. 1B, and at the start of beam 3 and
beam 4 in Fig. 1C). These observations likely indicate arching of the back. For
Patient A, the observation was made during 1 beam of 48 beams tested with LEILA.
For Patient B, the observation was made for 2 of 36 beams tested. While the
amplitude of the changes of the 3 LD parameters during these instances was small,
it is clear enough to implement a simple automated trend check during real-time
monitoring with LEILA, which alerts the operator of back arching.
Conclusion
Real-time
assessment of the quality of DIBH via the internal surrogates, the LD and SD
parameters at multiple levels in the radiation field, can help identify
situations where the patient arches their back instead of taking a sufficiently
deep breath-hold in DIBH breast
cancer treatments.
References
1.
Vasina E.N., Greer P., Thwaites D., Kron T., Lehmann J., A system for real-time
monitoring of breath-hold via assessment of internal anatomy in tangential
breast radiotherapy. Accepted to JACMP.
2. Bossuyt E, Weytjens R, Nevens D, De Vos
S, Verellen D. Evaluation of automated pre-treatment and transit in-vivo
dosimetry in radiotherapy using empirically determined parameters. phiRO. 2020 Oct 1;16:113-29.
Acknowledgements
This
work was supported by NHMRC grant 1147533.