Clinical evaluation of novel DWI sequence on rectal cancer patients in a low tesla MR-Linac system
PO-1619
Abstract
Clinical evaluation of novel DWI sequence on rectal cancer patients in a low tesla MR-Linac system
Authors: Matteo Nardini1, Amedeo Capotosti1, Giuditta Chiloiro2, Luca Boldrini2, Davide Cusumano1, Angela Romano2, Marco Valerio Antonelli2, Gabriele Turco2, Roberto Moretti1, Luca Indovina1, Maria Antonietta Gambacorta2, Vincenzo Valentini2, Lorenzo Placidi1
1Fondazione Policlinico Universitario Agostino Gemelli IRCCS, UOSD Fisica Medica e Radioprotezione, Rome, Italy; 2Fondazione Policlinico Universitario Agostino Gemelli IRCCS, UOC Radioterapia Oncologica, Rome, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Magnetic
resonance guided radiotherapy (MRgRT) allows online adaptation based on the
daily anatomy as well as on quantitative tissue variation. The latter aspect,
exploit the possibility to assess treatment response during each treatment’s
fraction, emplying quantitative imaging as MR diffusion weighted (DWI). The aim
of this study is to evaluate the use of DWI in a low tesla MR-Linac system to assess
any tissue variation during the treatment.
Material and Methods
Six patients enrolled in the
clinical trail (simultaneous integrated boost with two levels: 45 Gy to the
pelvis and 55 Gy to Gross Tumor Volume (GTV) plus the corresponding mesorectum)
have been included in this preliminary evaluation. This trial foresees a
primary tumor boost (60.1 Gy) from the third week of the treatment (from
fraction number 11) if patient shows an Early Regression Index (ERI) higher
than 13.1, which correspond to a prediction of not complete response. DWI is
acquired after treatment delivery on the central GTV slice during the
pretreatment simulation and each five fractions. DWI sequences has been
optimized for low tesla MR scanner accurately selecting parameters as: direction
of the diffusion (only slice direction), number of measurements, artifact noise
threshold reduction and number of b-value employed for the calculation of Apparent
Diffusion Coefficient (ADC) map. ADC map is then generated using ImageJ
software using a mono-exponential model. Results have been analysed in terms of
mean ADC values variation along the fractions for each patients. ADC values has
been computed not only on the GTV but also on the right femoral head (FH) as
reference for ADC constancy.
Results
Among the
six patients enrolled in this preliminary analysis, only two result to be not responder
(figure 1, continuous line). DWI were acquired within a maximum time of seven
minutes, with quite good compliance of the patients. ADC maps have been
computed off-line and analysed for each fraction (figure 1) in terms of ADC
values. GTV ADC value standard deviation (SD) is 0.6: 0.4 and 0.8 for “responder” and “not
responder”, respectively. Similarly, if considering right femoral head, the SD
is 0.08, while for “responder” and “not responder” is 0.09 and 0.05
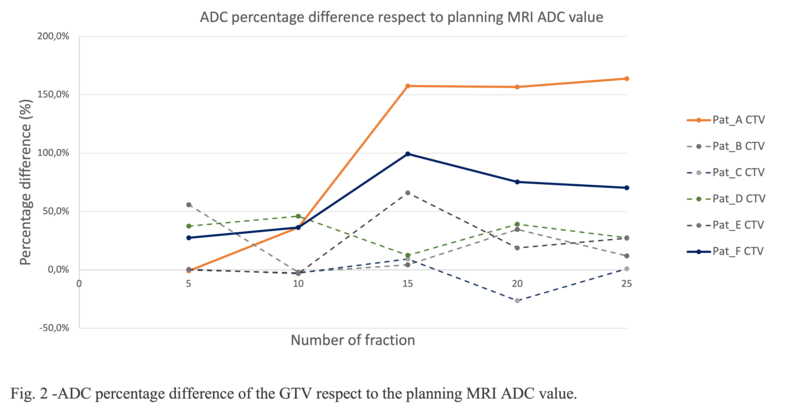
rispectively. Figure 2 shows the ADC percentage difference of the GTV with respect
to the simulation ADC value. ADC percentage difference between fraction 10 and
15 is always within 66% for “responder” and higher than 99% for “not responder”.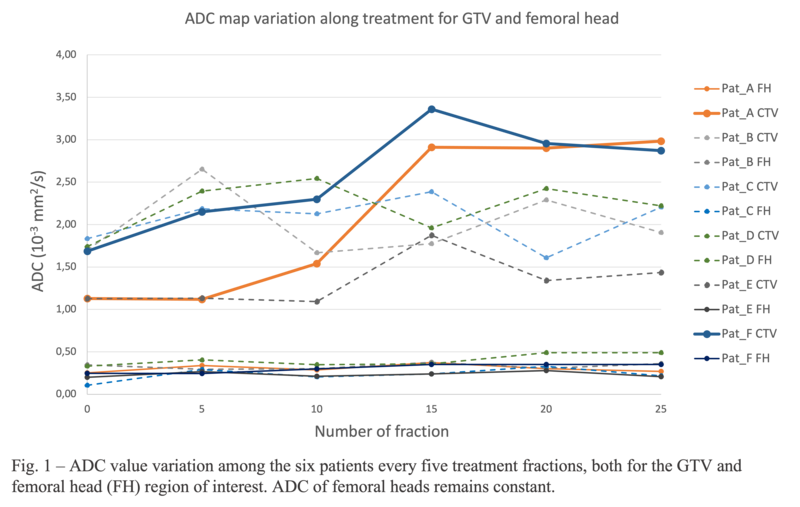
Conclusion
Even obtained
using a reduced number of cases, these preliminary results seem to highlight a different
behaviour of the GTV mean ADC values between “responder” and ”not responder”
patients included in this clinical trial. ADC values can potentially detect and
quantify GTV tissues variations caused to the ongoing treatment in a low field
MR-Linac system. Further analysis of the remaining 56 patients that will be
enrolled in the clinical trail, could confirm this promising preliminary results.