Development of simplified auto-segmentable functional cardiac atlas
PO-1600
Abstract
Development of simplified auto-segmentable functional cardiac atlas
Authors: Pierre Loap1, Ludovic De Marzi1, Krassen Kirov2, Vincent Servois3, Alain Fourquet1, Abdelhafidh Khoubeyb2, Youlia Kirova1
1Institut Curie, Department of Radiation Oncology, Paris, France; 2Institut Curie, Department of Anesthesiology, Paris, France; 3Institut Curie, Department of Radiology, Paris, France
Show Affiliations
Hide Affiliations
Purpose or Objective
There are increasing
evidences that radiation doses to specific cardiac substructures are associated
with cardiac adverse events. Manual delineation of cardiac substructures is
time consuming, and auto-segmentation
of cardiac substructure atlases has consequently been evaluated. However, proper
delineation of small substructures, such as the left anterior descending
coronary artery (LADCA), is challenging and conduction system substructures have
never been considered, despite frequent reports of radiation-induced
arrhythmias for thoracic irradiation. The aim of this study was to propose and
evaluate a simplified auto-segmentable functional cardiac atlas.
Material and Methods
We
created a cardiac substructure atlas from 20 breast cancer patients’ CT scans consisting
of the four cardiac cavities, of a high-risk cardiac zone (HRCZ) as a LADCA
surrogate and of the two cardiac conduction nodes. Performance evaluation of
atlas-based auto-segmentation (ABAS) was evaluated on a validation data set
consisting of 20 additional CT scans. Dice similarity coefficients (DSC) were
used to evaluate the concordance level between the manual and the automatic
segmentations.
Results
The average
duration of manual segmentation of the proposed cardiac atlas (illustrated in Figure
1) ranged between fifteen to twenty minutes, while ABAS lasted two minutes.
The median DSC for the delineated cardiac substructures was 0.718 (Figure 2).
The highest similarity between manual and automatic segmentation was observed
for the left ventricle with a median DSC of 0.87, while the lowest similarity
between manual and automatic segmentation was observed for the NAV with a
median DSC of 0.15. Regardless of the considered cardiac substructure,
auto-segmentation tended to result into smaller volumes than manual
segmentation . While smaller, the auto-segmented NAV and SAN were
systematically localized within the manual contours. The auto-segmented NAV
could be approximated by a 1.6-cm sphere and the auto-segmented SAN by a 1.0-cm
sphere.
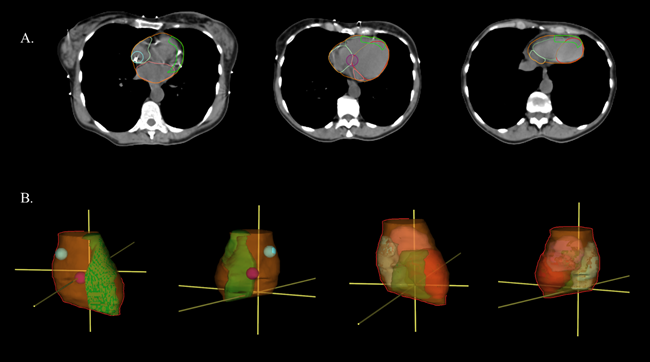
Figure 1: Simplified functional cardiac atlas. The left ventricle is delineated in red, the right ventricle in dark green, the left auricle in light green, the left auricle in pink, the high-risk cardiac zone in green, the SAN in blue and the AVN in purple. A. Axial plane. B. 3D representation.
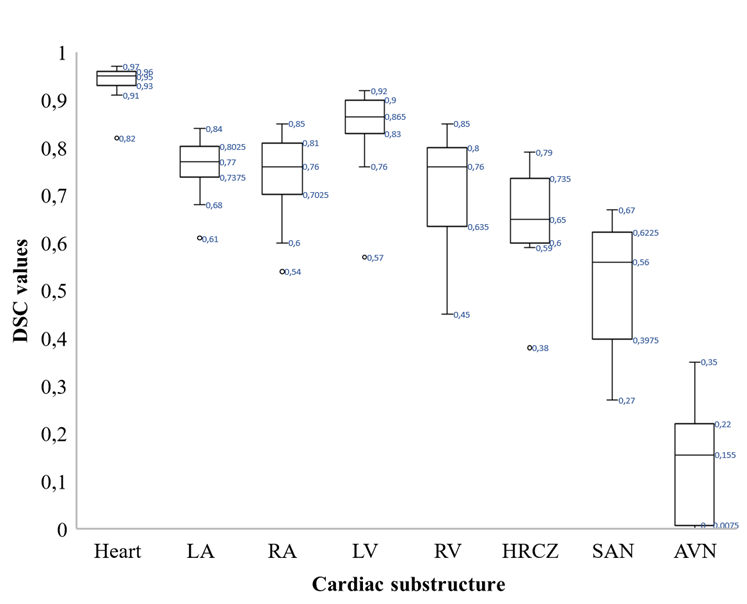
Figure 2: performance of atlas-based
auto-segmentation of the proposed simplified functional cardiac atlas. DSC: Dice Similarity Coefficient. LA : left auricle. RA : right auricle. LV : left ventricle. RV : right ventricle. HRCZ : high risk cardiac zone. SAN : sinoatrial node. AVN : atrio-ventricular node.
Conclusion
We proposed a simplified functional cardiac atlas, for which
coronary delineation difficulties were circumvent using a surrogate high risk
cardiac zone and cardiac conduction system was considered. Most cardiac
substructures were associated with acceptable ABAS properties. Such atlas could
be potentially evaluated for epidemiological studies and clinical practice.