Evaluation of an independent dose calculation software based on AAPM Task Group 219
PO-1537
Abstract
Evaluation of an independent dose calculation software based on AAPM Task Group 219
Authors: Juliana Dias1, Samuel Avelino1, Taís Peron1, Juliano Nakashima1
1Vitta - Centro de Radioterapia, Radiotherapy, Brasília, Brazil
Show Affiliations
Hide Affiliations
Purpose or Objective
Independent Dose Calculation Software (IDCS)
is an important safety tool in quality assurance programs. Considering that
AAPM TG 219 report was recently published to standardize the acceptance and commissioning
of IDCS, the present study applied this report to evaluate a commercial IDCS,
and to validate the method and action levels suggested.
Material and Methods
We
assessed DoseCHECK (Sun Nuclear, FL, USA) as an IDCS for our clinical Eclipse TPS,
v15.5 (Varian Medical Systems, CA, USA). The Eclipse was commissioned using the
Analytical Anisotropic Algorithm (AAA) for 6 and 10 MV of a Varian TrueBeam .
Based on AAPM TG 219, we evaluated 71 dose points per energy in order to
verify: PDP, profiles, dynamic wedges, field edges, surface region, simple IMRT
pattern (pyramid shape), and AAPM TG 119 IMRT plans. To evaluate high modulated
VMAT plans, we used a home-made heterogeneous phantom. The 19 irregular static
fields suggested by AAPM TG 219 were included in our analysis. We created
verification dose points at positions that considered the intent of each evaluation
plan. The dose range of the points tested varied from 200 to 600 cGy. We
exported all plans to the IDCS. We compared the doses calculated at all
verifications points by DoseCHECK (collapsed cone convolution algorithm), with
Eclipse and with ionization chamber and diode measurements (diode was used for
3x3 cm2 or smaller fields). We considered an action level of 5% for:
single beam/low gradient/homogeneous phantom; or composite beams/high gradient/
homogeneous phantom. In addition, we used an action level of 7% for: single
beam/high gradient/homogeneous phantom; or composite beams/high gradient/heterogeneous
phantom.
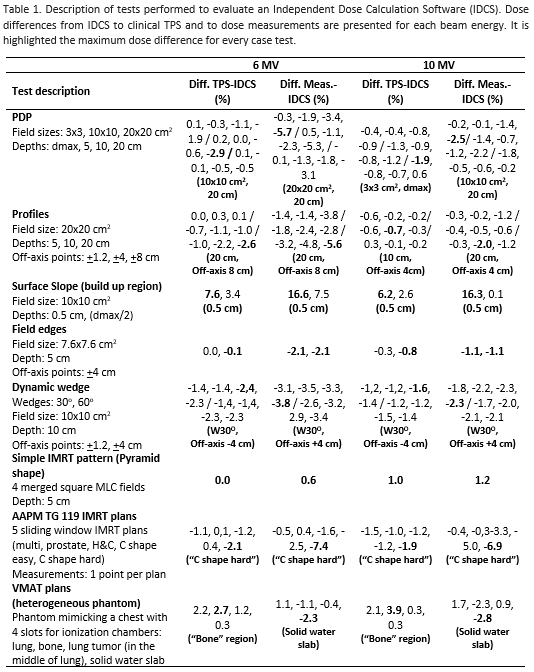
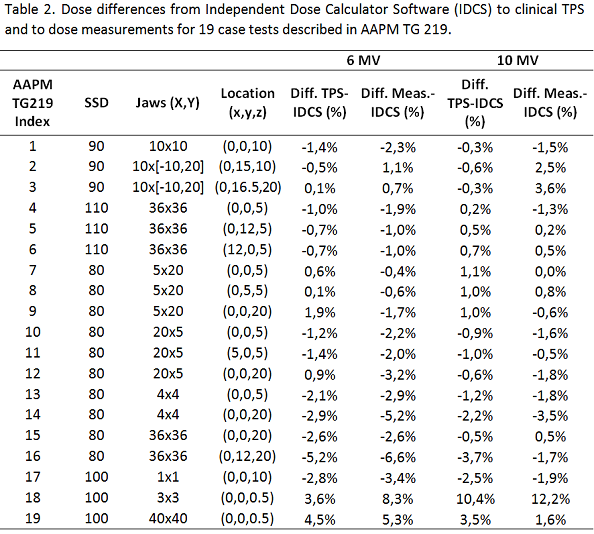
Results
The Table 1 shows the results of case tests performed based on AAPM TG 219. The Table 2 shows the results of the 19 specific case tests suggested by AAPM TG 219. For 6 MV beam, the IDCS deviated from TPS in 2 dose points and from measurements in 8 dose points. For 10 MV beam, the IDCS deviated from TPS in 1 dose point and from measurements in 3 dose points. In both sets of tests, the situations that did not respected the action levels suggested in AAPM TG 219 were at superficial points located 5 mm from the surface, at points located 20 cm depth, and in a 6 MV high modulated AAPM TG 119 plan. The tests with poor results slightly diverge from action levels considered or they are related to not clinically relevant points.
Conclusion
Our study reported good agreement among TPS, IDCS and measurements. The case tests with higher deviations occurred at regions with very high dose gradients or at deep depths. We consider very importantly to take into account more reports using the same methodology of AAPM TG 219, before we review the commissioning performed in our department. With more reports about uncertainties involved in independent dose calculation process, we expect that the action levels for dose points near surface (high dose gradient) could be reconsidered.