Commissioning of Total Body Irradiation and effect of beam spoiler distance on surface dose
PO-1522
Abstract
Commissioning of Total Body Irradiation and effect of beam spoiler distance on surface dose
Authors: BHARATH PANDU1, Khanna D2, Bharath Pandu3, Rajadurai Elavarasan3, Mohandass P4, Hima Nainan5, Vivek T R6
1Karunya institute of technology and sciences, Department of Applied Physics, Coimbatore, India; 2Karunya Institute of technology and sciences, Department of Applied Physics, Coimbatore, India; 3Bangalore Baptist Hospital, Department of Radiotherapy, Bangalore, India; 4Fortis Hospital, Department of Radiation Oncology, Mohali, India; 5Bangalore Baptist Hsopital, Department of Radiotherapy, Bangalore, India; 6Tawam Hospital, Department of Radiation Oncology, Abu dhabi, United Arab Emirates
Show Affiliations
Hide Affiliations
Purpose or Objective
The aim of the current study is to compare surface dose while varying the
distance between beam spoiler and phantom surface as well as commissioning of
compensator based Total Body Irradiation (TBI).
Material and Methods
Elekta Synergy®Platform™ treatment unit with 6MV photon beam, gantry
angle 270°,
collimator angle 45° and field size 40x40 cm2, SSD at 385cm was set up for this study. The TBI commissioning was performed for the bi-lateral extended SSD
treatment technique. Beam spoiler made by Acrylic sheet of 1.0cm thickness used
for percentage depth dose (PDD) measurement at 10cm, 20cm, 30cm and 40cm from
the phantom surface to evaluate dose at maximum depth (Dmax). All the measurements
were carried out with the acrylic phantom size of 30x30x30cm3 using a Parallel plate (PPC40) and Farmer (FC65) ion chamber for depth ranging from
0.1cm to 1.5cm and 1.0cm to 24.0cm with water cans on both sides to account for
lateral scatter. As a part of TBI commissioning, beam profile measurements and
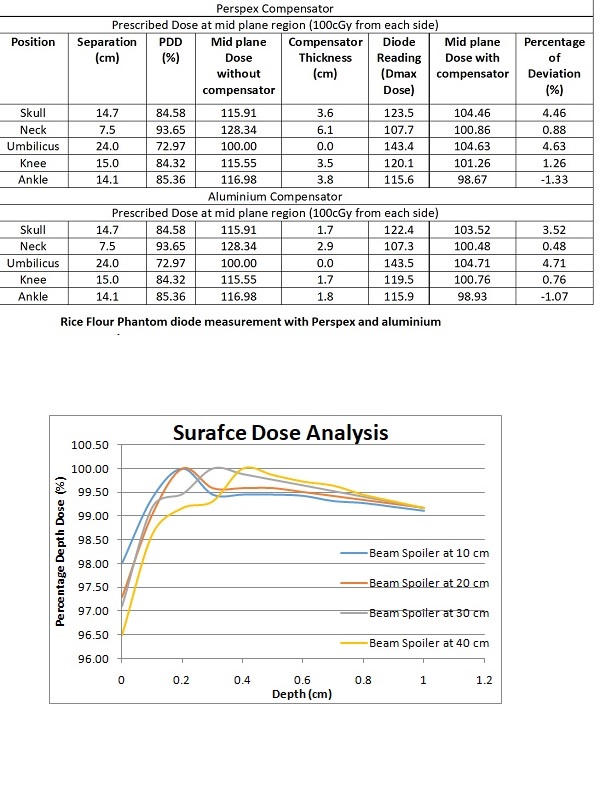
HVL were performed using both Perspex (Prpx) and Aluminium (Al) material. An
in- house Rice flour (RF) phantom was customized with different anatomical
regions such as head, neck, shoulder, umbilicus, thigh, knee and ankle for
quality assurance purpose. The separation of each anatomical region was
measured using a vernier calliper for calculating Monitor units and thickness of the compensator. The calculated MU was delivered while keeping Prpx or Al
compensators to compensate for varying thickness of the phantom body. In
addition, In-Vivo Diodes (IVD) were placed on the different regions of the RF
phantom to measure the delivered measured dose which is compared with the calculated
dose for validation.
Results
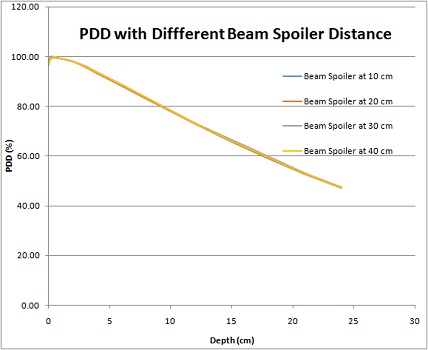
The results of PDD revealed
that the measured surface dose varies with the distance of the beam spoiler from
the phantom surface. An increased Dmax and surface dose was observed when the beam
spoiler moved from the phantom surface. The Dmax was observed 0.2cm
at 10cm and 20cm distance. Similarly, the Dmax was found to be
0.3cm, 0.4cm at 30cm and 40cm. The flatness and symmetry of the beam profile
were observed at 104.8% and 100.2%. In addition, a half-value layer of Prpx and Al was
17cm and 8cm respectively. The percentage of deviation between the measured and
calculated dose of each anatomical region was less than ±4.7%
for both Prpx and Al.
Conclusion
The present study concluded
that to achieve a uniform dose to the whole body during TBI, the beam
spoiler can be kept at an optimum distance ranging from 10cm to 20cm to get the
desired skin dose. After successful commissioning and measurement validation,
we could establish a compensator based TBI technique for Elekta Synergy®linac.