Simplified models for radiotherapy-induced lung cancer risk evaluation in breast treatment
PO-1511
Abstract
Simplified models for radiotherapy-induced lung cancer risk evaluation in breast treatment
Authors: Alessia D'Anna1, Giuseppe Stella1, Elisa Bonanno2, Giuseppina Borzì3, Nina Cavalli3, Andrea Girlando4, Anna Maria Gueli1, Martina Pace5, Lucia Zirone5, Carmelo Marino6
1University of Catania, Department of Physics and Astronomy "E. Majorana", Catania, Italy; 2Humanitas - Istituto Clinico Catanese, Department of Medical Physics, Misterbianco , Italy; 3Humanitas - Istituto Clinico Catanese, Department of Medical Physics, Misterbianco, Italy; 4Humanitas - Istituto Clinico Catanese, Department of Radiotherapy , Misterbianco, Italy; 5University of Catania, School of Medical Physics, Catania, Italy; 6Humanitas - Istituto Clinico Catanese, Department of Medical Physics, Catania, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Conserving surgery followed by external beam
radiotherapy is considered the "Gold Standard" for early stage of
breast cancer. This approach may introduce an excess risk for second cancer
induction due to breast exposure to therapeutic doses. The aim of this study was
to estimate radiotherapy-induced lung cancer risk and to propose simplified
models useful in clinical routine to reduce it in a preventive way during the
treatment planning phase.
Material and Methods
Using
the Schneider Mechanistic Model, radiotherapy-induced lung cancer risk for
breast cancer has been estimated for 288 patients (aged between 30 and 70
years) treated with Three-Dimensional Conformal Radiation Therapy and Standard Fractioned
(3D-CRT SF) at Humanitas - Istituto Clinico Catanese (H-ICC) (Catania, Italy). Organ
Equivalent Dose (OED), Excess Absolute Risk (EAR), Lifetime Attributable Risk
(LAR) and Relative Risk (RR) values has been calculated implementing a Script
(C# language) through the Varian Eclipse Scripting Application Programming
Interface (ESAPI). Statistical parameters have been provided by several sources:
H-ICC, Istituto Nazionale di Statistica (ISTAT) and Integrated Cancer Registry
CT-ME-EN. Using a C++ code, simulations have been performed on the whole
statistical sample imposing an attained patient’s age (agea) equal
to 75 Y and an age of the patient during exposure (agee) varying
between 30 and 70 years in steps of 5 years. In order to minimise the
difference between LAR from Schneider model (LARSchneider) and LAR
from simplified model a parameter optimisation process has been performed,
i.e., a minimization of Mean Square Error (MSE).
Results
The first step was to
fit linearly LAR values as a function of OED for i-th agee (i = 30,
35, …70) (1), where ai is the i-th angular
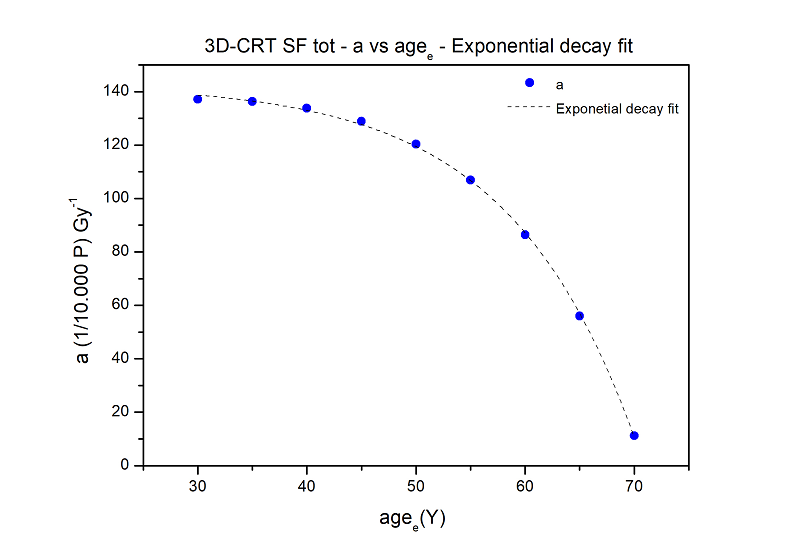
coefficient for the i-th agee. he next step was to
relate the growth rate of the LAR to the time range agee-agea (fig.).The analytic
relationship (R2=0.99) found was (1). Substituting
(2) to (1) we obtained the simplified model named OSM (3). OSM optimised parameters
obtained after optimisation process
were: A=-0.340 [(1/10000 P) Gy-1], B=-11.688 [Y], C=144.557 [Gy-1].
The percentage differences (Δ%)
between LARSchneider and LAROSM values were < 2%. A
linear relation (R2=0.96) was found between OED and V4 (% lung
volume absorbing a dose of 4 Gy) (4). Substituting
(4) to (3) we obtained the simplified model named VSM (5). VSM optimised parameters obtained, after optimisation process were: A=-0.300 [(1/10000 P) Gy-1],
B=-11.387 [Y], C=147.601 [Gy-1], M=0.830 [(1/10000 P) Gy-1],
N =0.069 [Y]. The percentage
differences (Δ%) between LARSchneider and LARVSM values
were < 5%.
Conclusion
This study provided three
different tools for risk calculation: Eclipse™ script, OSM and VSM. These, in
different ways, allow the medical physicist to quickly obtain LAR values for
each treatment plan, which is why they could easily be used in clinical
practice.