Robustness evaluation of ultra hypo-fractionated IMPT for PCa on target and OAR dose-constraints
Senquan Feng,
Netherlands Antilles
PO-1500
Abstract
Robustness evaluation of ultra hypo-fractionated IMPT for PCa on target and OAR dose-constraints
Authors: Senquan Feng1, Charlotte Brouwer1, Erik Korevaar1, Neha Vapiwala2, Kang-Hsin Wang3, Curtiland Deville4, Johannes Langendijk1, Stefan Both1, Shafak Aluwini1
1University of Groningen, University Medical Center Groningen, Department of Radiation Oncology, Groningen, Netherlands Antilles; 2University of Pennsylvania, Department of Radiation Oncology, Philadelphia, USA; 3UT Southwestern, Department of Radiation Oncology, Dallas, USA; 4Johns Hopkins University School of Medicine, Department of Radiation Oncology and Molecular Radiation Sciences, Baltimore, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
Intensity modulated proton therapy (IMPT) for
prostate cancer (PCa) is susceptible to inter- and intra-fraction organ
movement. Its dosimetric impact can be magnified by hypo-fractionation. In
general, proton treatment plans are robustly evaluated against setup and range
uncertainty. This study proposes a method
to evaluate the dosimetric impact of inter- and intra-fraction prostate motion in
ultra hypo-fractionated IMPT for PCa. Results will be compared against the
general robustness evaluation approach.
Material and Methods
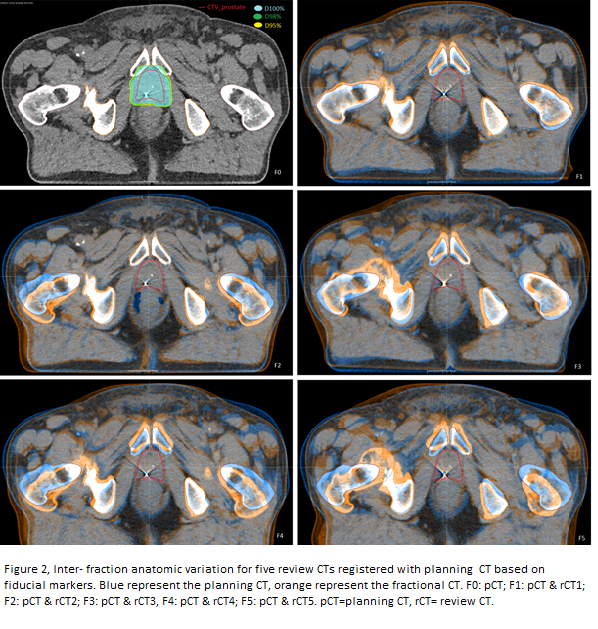
One representative PCa patient treated in our
medical center, presenting typical inter-fraction motion(Figure 2) based on
fiducial marker registration between five consequential review CT images, was included
in this study. IMPT plans were generated
using two lateral opposed beams and robust optimization settings of
3%/5mm (Raysearch, 8.99). Plans were clinically accepted when fulfilling
voxel-wise worstcriteria for CTV coverage using 5-mm setup and +/-3%
range uncertainty, plans were accepted if the dose parameters were within max 5%
deviation of constraints. Each proton beam was splitted into 14
sub-plans in accordance with energy layers and time of beam delivery (one sub-plan
per second and per energy layer). Electro-magnetic detected prostate motion was
summarized from 26 PCa patients treated in the department of radiation oncology
of the University of Pennsylvania, and 8 maximum motion vectors (diagonal directions) covering 95%range of prostate movement were created, with
max motion vector of 5.4mm. In each fraction of every scenario, a synthetic CT
was created from the corresponding review CT and randomly selected prostate motion
vector with random duration of movement using deformable image registration with
controlling ROIs in RayStation 7.99 Research. Figure 1 shows one example treatment
simulation of prostate motion trajectory in five fractions of treatment. In
total, 20 treatments were simulated based on 40 synthetic CTs. For each
treatment simulation, the five resulting fractional doses were warped back and
accumulated dose was presented at the planning CT.
Results
The nominal, voxel wise worst-case and accumulated dose of the simulated scenarios is presented in Table 1. In terms
of target coverage, simulated accumulated doses were higher than the voxel wise
worst-case dose in 19 out of 20 simulations. For OARs, all
simulated accumulated doses were lower than the voxel wise worst-case dose. The
largest difference between nominal vs. voxel wise worst vs. simulated
accumulated dose was found for the posterior rectal wall (1898 cGy vs. 3026 cGy
vs. 2675 cGy, respectively), highlighting the importance of plan evaluation
using a voxel-wise worst case evaluation.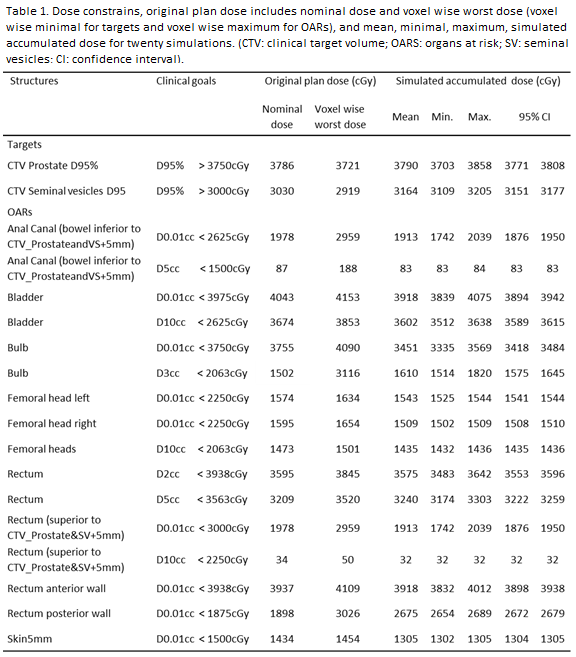
Conclusion
Evaluation of ultra hypofractionated IMPT for PCa by a voxel wise worst-case approach using 5-mm
setup and 3% range uncertainty is found to be robust
for the anticipated target coverage and OAR dose for at least 95% of
intra-fraction prostate movement found in clinical practice.