Dosimetric impact of bladder changes in prostate VMAT based on dose deformable image registration
Alicia Gonzalez Pose,
Spain
PO-1491
Abstract
Dosimetric impact of bladder changes in prostate VMAT based on dose deformable image registration
Authors: Alicia Gonzalez Pose1, Beatriz Vázquez Barreiro2, Julio Santiago Vázquez Rodríguez1, Benito Andrade Álvarez1, Antonio Teijeiro García1, Ana Belén Blanco Ledo2, Mercedes Riveira Martin3, Ricardo Dorado Dorado1, Antonio López Medina1, Manuel Salgado Fernández4
1Hospital Meixoeiro, Medical Physics, Vigo, Spain; 2Hospital Meixoeiro, Radiation Oncology, Vigo, Spain; 3Galicia Sur Biomedical Foundation, Health Research Institute, Vigo, Spain; 4Hospital Meixoeiro, Medical Phyisics, Vigo, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
To
investigate dosimetric impact of prostate radiotherapy sessions
delivered with a bladder volume smaller than the planned. Based on
CBCT dose deformable registration, it is possible to establish a
criteria about how many sessions with non-optimal bladder filling
are possible to avoid CBCT repetitions. This would be helpful to
avoid overdoses and to optimize treatment schedules and resources,
resulting in a specific offline protocol for prostate cancer VMAT
EBRT.
Material and Methods
We
evaluated daily CBCTs of 23
patients treated with EBRT (VMAT 6MV ClinacIX). The prescribed doses
were 57.6
7.5 Gy to the prostate or prostate bed and 44.74
0.58 Gy to the CTV encompassing prostate or prostate bed and regional
pelvic lymphatics nodes. All patients were classified in 6 groups of
4 patients depending on the number of sessions in which CBCT
repetition due to different bladder filling was necessary: from none
to five sessions.
A
dose deformable image registration computed with Velocity software
(Varian) was used to obtain full treatment dosimetry. All non-optimal bladder
sessions calculated
(Eclipse v15.6.06 TPS)
on their unfavourable CBCTs were added. The optimal bladder sessions
were grouped every five and calculated on one CBCT chosen as
representative. Bladder,
rectum , prostate CTV and pelvis CTV were contoured in each one. The
mean dose (Dmean) and V40 of bladder and rectum, as well as the D95
of both CTVs were assessed. The dose differences between planned and
registered treatment volumes were calculated (difference = registered
- planned).
Finally, this difference was evaluated for every patient group with
the mean and standard deviation. Dose constraints were based on RTOG
0415 dose limits.
Results
The
mean ratio in bladder volume between planned CT and CBCT (bladder
planned/bladder CBCT) was 1.2
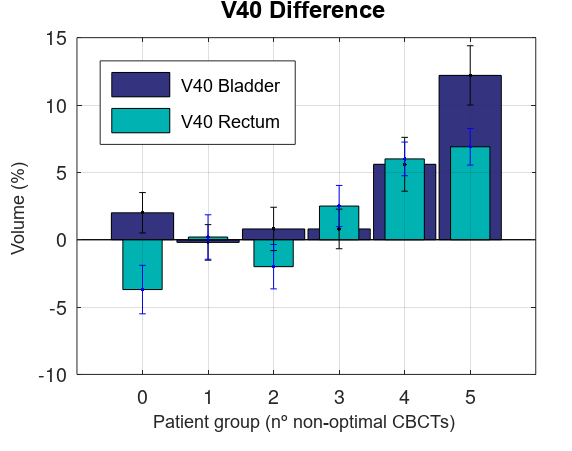
0.4. Differences between calculated and planned Dmean for rectum and
bladder were always less than 5 Gy. Admissible variations in V40 in
rectum (-1.8
1.7 %) and bladder (0.8
1 %), also a better CTVs coverage have been reached in no- repeated
CBCT and CBCT repeated once. Groups in where 2 and 3 CBCTs were
repeated, a slight increase of the V40 in bladder was found (0.9
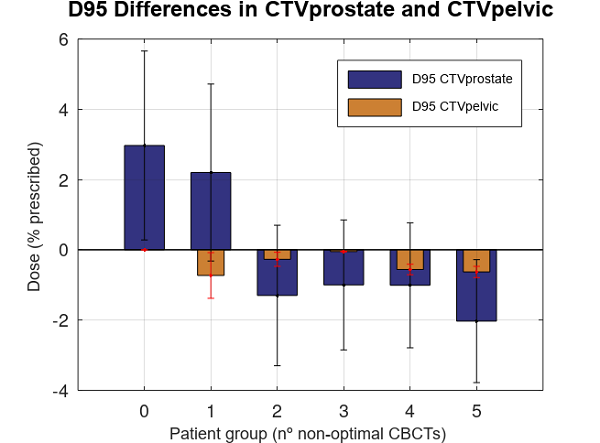
1.1 %) along with an underdose
of pelvic CTV (D95 -0.2
0.4 % prescribed dose) and prostate CTV (D95 -1.1
1.9 % prescribed dose) . Finally, for groups of 4 or more
non-optimal CBCT, a significant increased was observed in V40 of
bladder (8.9+-6.3 %) and rectum (6.3 +-2%), underdosing
both CTVs (D95 CTV prostate -1.3 +-2 % prescribed dose) and CTV
pelvic /-0.67 +- 0.35 % prescribed dose).
Conclusion
According
to our results, the dose deformable CBCT registration
could report that
smaller
bladder volume
than planned is
allowed until 3 times with permissible dose tolerance in bladder and
rectum also a correct CTV’s coverage. Futures
applications of our results will be the creation of a specific
offline protocol.