Exploring published acute esophagitis models to support improved clinical management in thoracic RT
PO-1250
Abstract
Exploring published acute esophagitis models to support improved clinical management in thoracic RT
Authors: MARIA THOR1, Ellen Yorke1, Jean M Moran1, Bobby Daly2, Daniel R Gomez1, Joseph O Deasy1
1Memorial Sloan Kettering Cancer Center, Medical Physics, NEW YORK, USA; 2Memorial Sloan Kettering Cancer Center, Medicine, NEW YORK, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
Acute esophagitis (AE) is associated with discomfort and may lead to treatment interruption. The goal of this work was to explore published AE models in an independent thoracic cancer cohort treated with hypofractionated radiotherapy (RT) and define dose-volume histogram (DVH) thresholds associated with high AE risk in order to identify patients for more intensive monitoring and symptom management.
Material and Methods
PubMed was searched for published models relating to ≥grade 2 AE (AE2+). Models were explored in 138 internally accumulated thoracic patients that received RT alone in 15 fractions (3Gy or 4Gy/fraction) between January 2019 and March 2021 after correcting the esophagus doses for fractionation effects (using a/b=10Gy). The AE2+ rate was 19%. Calibration and discrimination of the published models was assessed (Hosmer-Lemeshow p-value (pHL) and AUC), and the DVH threshold was defined at the dose level prior to the steepest part of the dose-response curve and at which the first AE2+ case was observed.
Results
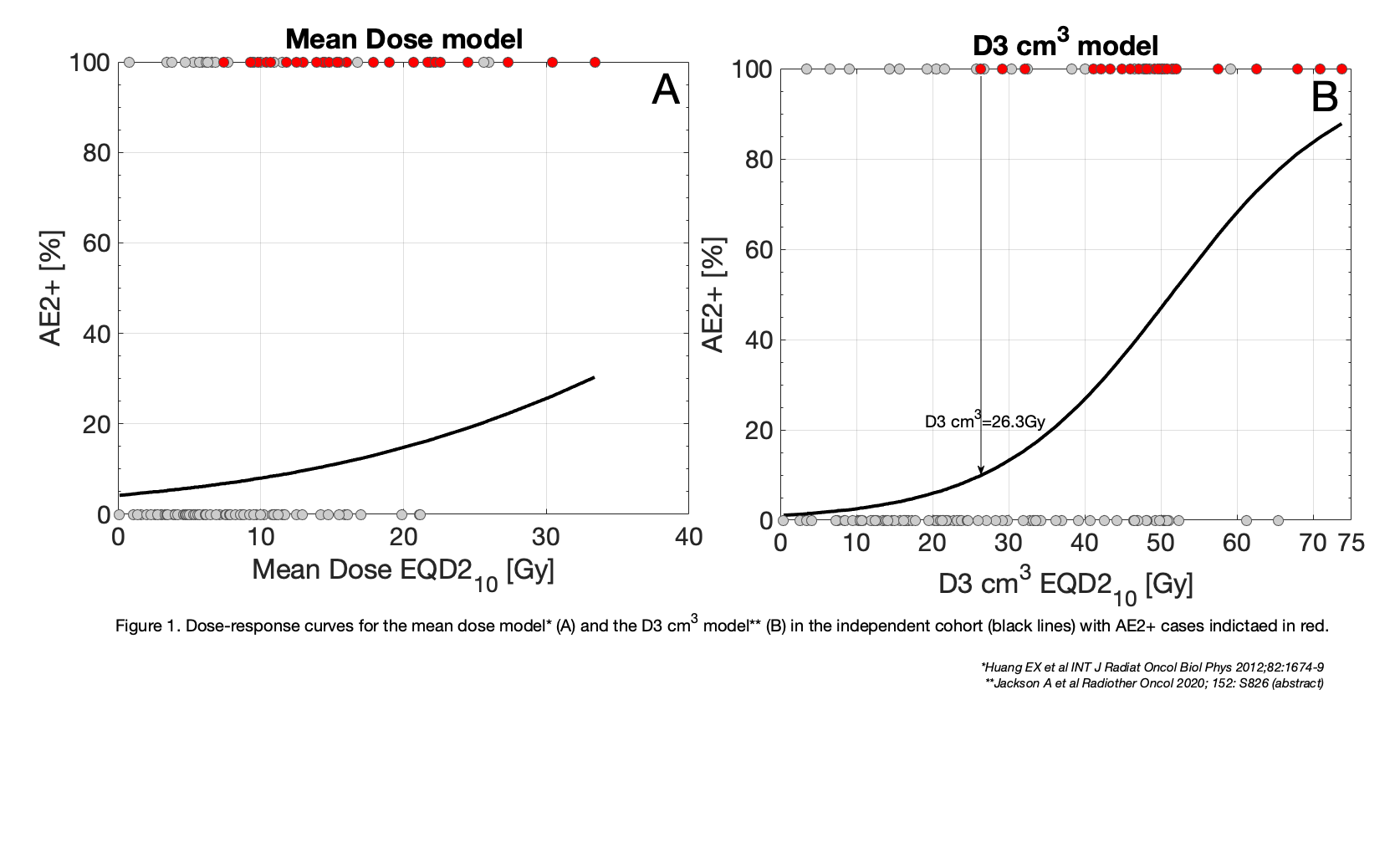
One mean dose model and one D3 cm3 model were identified. Both models correctly distinguished AE2+ with high reliability (Mean dose, D3 cm3 models: AUC=0.89, 0.85), but only the D3 cm3 model was well calibrated to data (pHL=0.26; Figure 1), and yielded a much steeper dose-response curve. The associated DVH threshold was 26 Gy in EQD2a/b=10Gy and was located at a predicted AE2+ rate of 9.8%. This DVH threshold has been internally incorporated as an action level for recruitment to the AE intervention program for all patients receiving thoracic RT in 15 fractions. During the first month of roll out, 5 patients have been identified for high risk of AE (median fractionation-corrected D3 cm3: 49 Gy) and thus enrolled for further intervention. Of these, four patients have developed AE2+.
Conclusion
We present results on the validation of published models to be used directly in clinical decision-making to reduce the rate of AE2+, improve overall outcomes, care and cost effectiveness of hypofractionated thoracic RT. So far, four of the five patients that were indicated by the developed D3 cm3 action level and recruited to the intervention program, have developed AE2+.