CECT vs. MRI: Impact of concordance index for gross target volume in IMRT of head and neck cancers
PO-1082
Abstract
CECT vs. MRI: Impact of concordance index for gross target volume in IMRT of head and neck cancers
Authors: Pallavi Kalbande1, Bharti Mahindrakar Jain2, Ashok Singh3, Nilavarasu Shanmugam4, Pournima Kale5, Zatin Mathi1, Bhagyashree Borikar6, Atul Tayde7, Niloy Ranjan Datta2
1Mahatma Gandhi Institute of Medical Sciences, Radiotherapy, Wardha, India; 2Mahatma Gandhi Institute of Medical Sciences , Radiotherapy, Wardha, India; 3Mahatma Gandhi Institute of Medical sciences , Radiotherapy, Wardha, India; 4Mahatma Gandhi Institute of Medical , Radiotherapy, Wardha, India; 5Mahatma Gandhi Institute of medical Sciences , Radiotherapy, Wardha, India; 6Mahatma Gandhi Institute of Medical Sciences , Radiology, Wardha, India; 7Mahatma Gandhi Institute of Medical Sciences, Radiology, Wardha, India
Show Affiliations
Hide Affiliations
Purpose or Objective
Radiotherapy (RT) forms an integral component of
management in head and neck cancers. Accurate delineation of GTV is a key step
of RT treatment planning. Target delineation is usually based on contrast
enhanced computed tomography (CECT) images and RT doses in IMRT are usually
prescribed to GTV of primary (GTVp) and nodes (GTVn). Magnetic resonance
imaging (MRI) offers the best soft tissue contrast to define primary tumor and
nodes when compared to CECT. As synthetic CECT from the MRI is usually
unavailable in RTP (radiotherapy treatment planning systems), RT planning is
mostly based on CECT volumes. We therefore, carried out this study to evaluate
concordance between CECT and MRI defined target volumes and corresponding dose-volume
histogram (DVH) parameters.
Material and Methods
10 consecutive unoperated patients of head and
neck cancer were included. All patients underwent CECT for RT simulation. In
addition, T1, T2 and T1C MRI images with similar slice thickness as of CECT
were obtained. GTVp and GTVn were delineated independently by two radiation oncologists
on CECT and MRI images and entire sets of contours. These were reviewed jointly
by another group of two radiation oncologists and radiologist. GTVp and GTVn
were included in high-risk volume, adjacent nodal levels were taken in
intermediate-risk volumes, while prophylactic nodal levels were included in
low-risk volume. Corresponding PTVs were generated and IMRT planning was done. Three
dose levels of 70 Gy, 63 Gy, 56 in 35 fractions over 7wks at 98% of dose
coverage of corresponding planning target volume (PTVs) were prescribed. The
DVH parameters evaluated for PTV were D2, D95, D98,
V95 and V100 for both CECT and MRI based target volumes. In
addition, %differences of GTVp, GTVn, GTVpn were computed along with concordance
index (ConI), conformity index (CI) and homogeneity index (HI). ConI was
ideally taken as 1.
Results
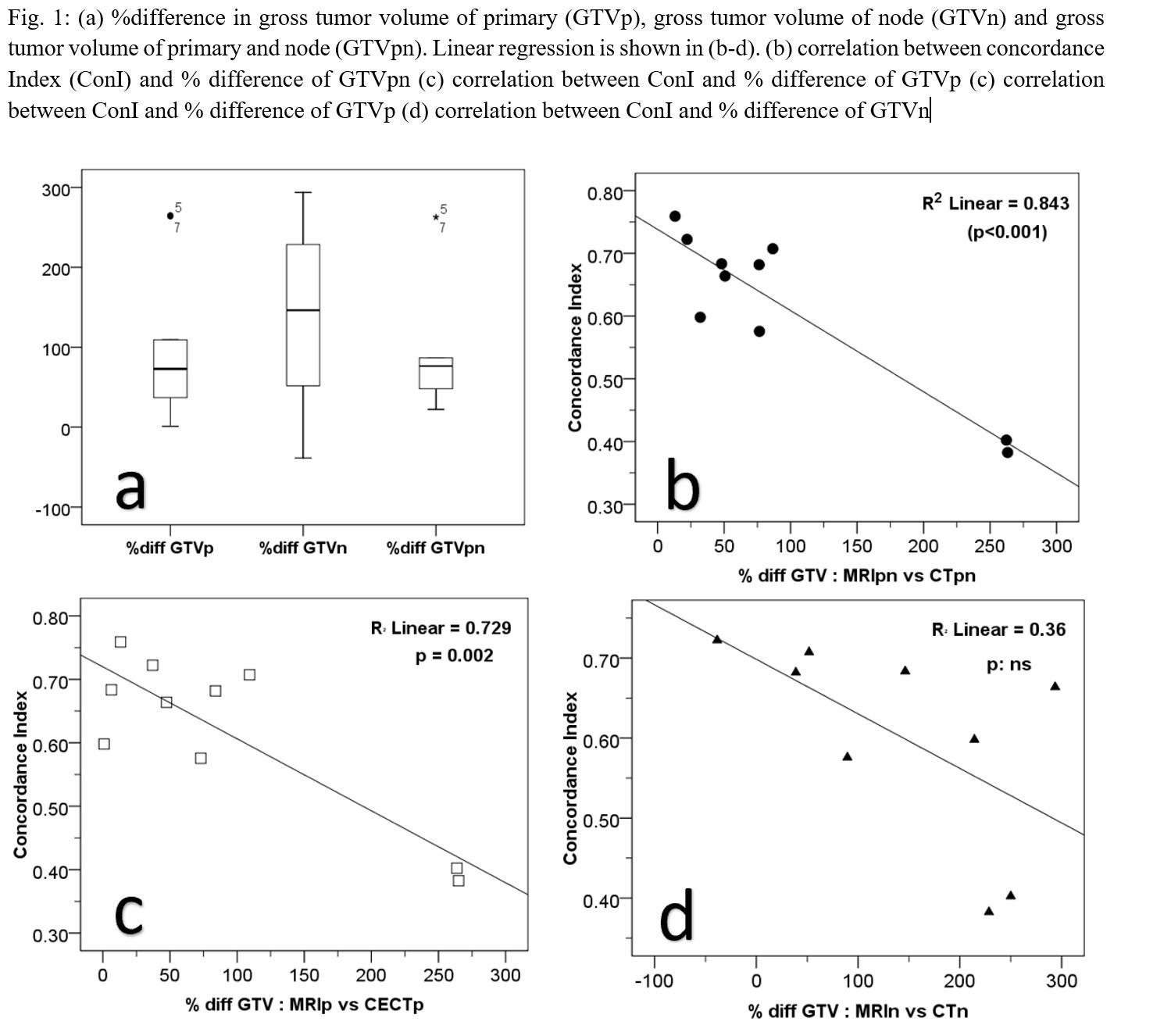
GTVp
and GTVpn delineated on MRI was found to be significantly higher than the corresponding
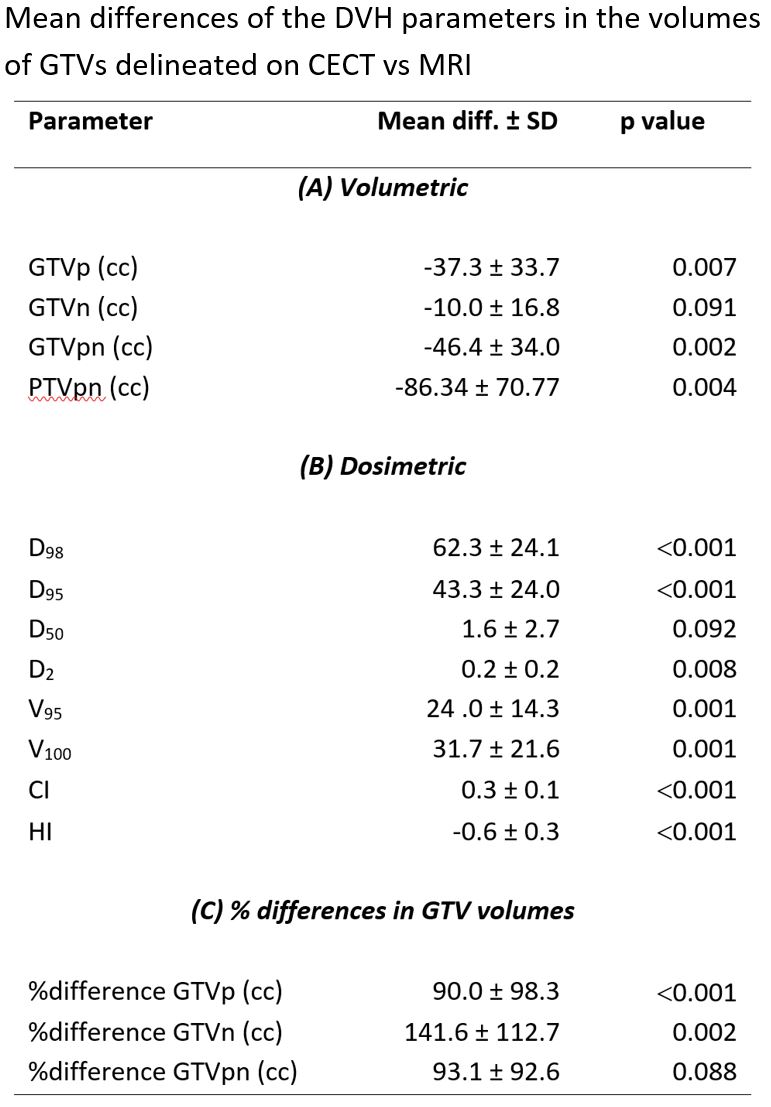
GTVs delineated (Fig). This resulted in significant
differences in the D2, D95, D98, V95,
V100, CI and HI (Table). %differences of GTVp and GTVn of
corresponding volumes delineated on CECT and MRI were significantly different. The
mean ConI was 0.6 (±0.1) (p=0.01) and was inversely
related to the %difference in GTVp (p=0.002) and GTVpn (p<0.001). For GTVn, a
similar trend was observed. Concordance of GTVpn varied from good (ConI,
≥0.67, n=5), moderate (ConI 0.34-0.66, n=4) and poor (ConI ≤0.33, n=1).
Conclusion
The GTVs and corresponding PTVs were
significantly larger on MRI than on CECT. This resulted in significant lack of concordance
of these two volumes. Thus, IMRT plans based solely on CECT delineated target
volumes could result in significant cold spots in the GTV/PTV, loss of
conformity and homogeneity. Thus, target delineations for head and neck cancers
should be ideally based on integration of CECT and MRI images to minimize these
dose discrepancies that could result in unsatisfactory locoregional control.