The geometric
stability of the high uptake volumes was high, with median (min;max) values of
OF01 : 0.83 (0.42;1.00) and
OF02 : 0.82 (0.38;1.00).
OF01 and OF02 for all patients are shown in fig1.
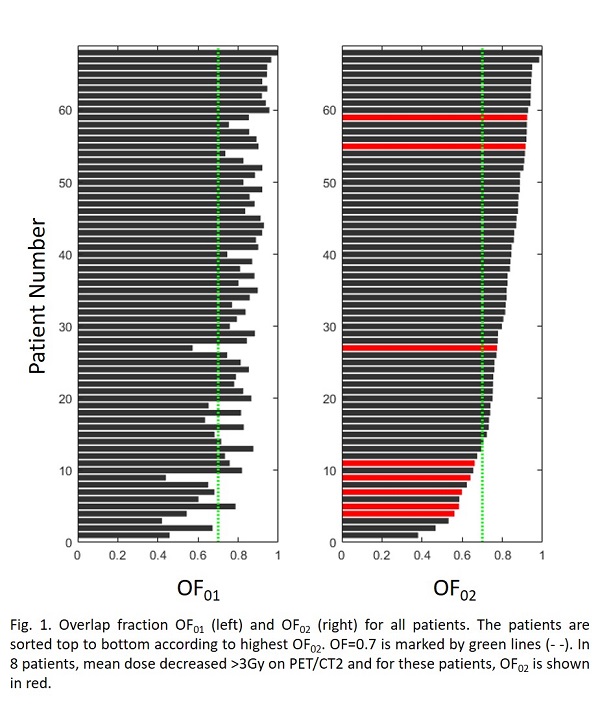
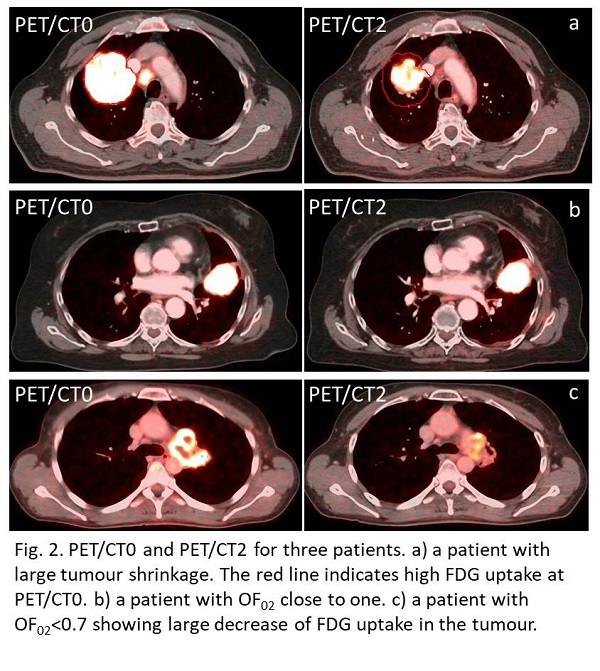
In 56 (82%) and 55 (80%) of the patients, the OF was above 0.7 at
PET/CT1 and PET/CT2, respectively. Both increase (negative ΔDV0,V2)
and decrease (positive ΔDV0,V2) in dose to V2 compared to V0 were
observed. Increase was in general due to tumour shrinkage as illustrated in
fig2a. There was a significant correlation between patients with OF02<70%
and patients with mean dose decrease >3Gy (p<0.001). Patients with
>3Gy decrease are highlighted in fig1. For patients with OF02 above
0.7, the median change in dose, ΔDV0,V2, was 0.2Gy(-4.4;5.5),
and in only 5% of these patients (3/55) the dose decrease >3Gy. For the 13
patients where the OF02 was below 0.7, the median change in dose, ΔDV0,V2,
was 2.1Gy(-0.9;17.0), and in 38% of these patients (5/13) the dose decreased
>3Gy.
The primary cause for OF02<0.7 was the decline of SUVpeak
to ~2 times background activity, as this resulted in large changes of the
region included in V2 for 54% of patients (7/13), see example in Fig 2c.
Additionally, OF02<0.7 was observed for patients with larger
anatomical changes, such as necrotic regions partly dissolved and changing atelectasis,
where plan adaptation was warranted.