Atlas-based auto-segmentation of pelvic CTVs in FDG-PET-CT planning of anal cancer
Marciana Nona Duma,
Germany
PD-0498
Abstract
Atlas-based auto-segmentation of pelvic CTVs in FDG-PET-CT planning of anal cancer
Authors: Marciana Nona Duma1, Max Bieder2, Markus Böhm3, Martin Freesmeyer4, Robert Drescher5, Steffen Weimann1, Andrea Wittig2
1University Hospital Jena, Department of Radiotherapy and Radiation Oncology, Jena, Germany; 2University Hospital Jena, Department of Radiotherapy and Radiation Oncology , Jena, Germany; 3University Hospital Jena, Institute for Medical Statistics, Computer Science and Data Science (IMSID), Jena, Germany; 4University Hospital Jena, Clinic of Nuclear Medicine, Jena, Germany; 5University Hospital Jena, Clinic of Nuclear Medicine , Jena, Germany
Show Affiliations
Hide Affiliations
Purpose or Objective
Several studies have evaluated the use of atlas-based auto-segmentation
(ABS) in different regions, mostly for organ at risk (OAR) delineation, while
the evidence for its performance in the pelvis, i.e. the clinical target volume
(CTV) is poor. This study aims to evaluate ABS in patients with anal cancer for
different ABS template-sizes.
Material and Methods
51 patients(pts.) with anal cancer who underwent 18F‑fluorodeeoxyglucose positron emission
tomography/computed tomography (FDG-PET/CT) radiotherapy treatment planning
were selected. All patients were scanned at the FDG-PET/CT scanner in treatment
position and the treatment planning was performed on the CTs of the FDG-PET/CT.
27/51 pts. had FDG-PET positive lymph node metastases (LN). The positive LNs
(n=27), as well as the CTV (n=51) according to the UK NATIONAL GUIDANCE FOR
IMRT IN ANAL CANCER (V4.07/12/2016) were retrospectively delineated in RayStation
(RaySearch Laboratories, Stockholm, Sweden). From the 51 contoured datasets one
ABS-template was created. A crucial parameter for the ABS is the number datasets
included in the algorithm. Five different
template sizes were assessed (ABS10=10 datasets within the template, ABS20, ABS30,
ABS40 and ABS50) to automatically delineate the CTVs of the 27pts with PET-positive
LN, with exclusion of their corresponding dataset from the ABS template.
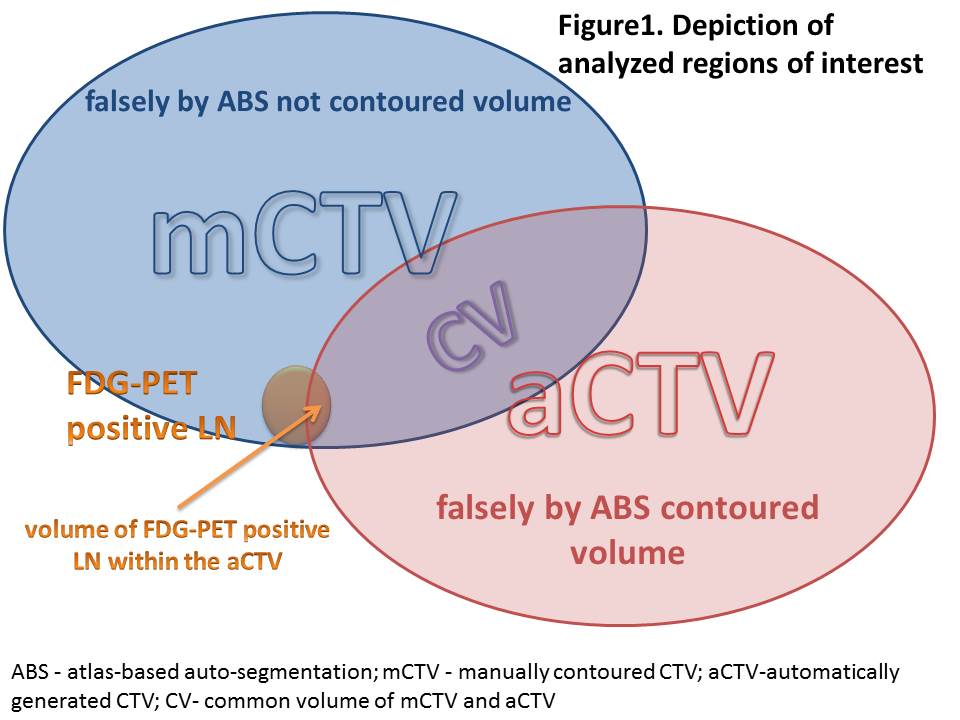
We evaluated:
- the dice similarity index (DSI) = 2xCV/ (mCTV+aCTV),
- the volume falsely not covered, as well as the volume falsely covered by
the aCTV,
- the volume of the PET-positive LN covered by the aCTV(Fig.1).
Friedman Test Post-hoc analyses were performed (SPSS Inc., Chicago, IL, USA).
A value of P<0.05 was considered to be statistically significant. We report median(range).
Results
In total, 103 LN were contoured. The LN were localized
in the inguinal (n=53;51%), external iliac (n=14;14%), internal
iliac(n=20;19%), mesorectal(n=10;10%) and presacral(n=6;6%) regions,
respectively. There was a slightly higher accuracy of aCTVs with increasing
numbers of pts within the template. For a statistically significant improvement
of the DSI an ABS40 (as compared to an ABS10) was necessary (Bonferroni-adjusted
p=0.017). There was no difference between ABS40 and ABS50 (DSI 0.795(range:0.705-0.847)
and 0.796(0.718-0.850), respectively). With rising numbers of datasets within
the template, the amount of falsely contoured and falsely not contoured volumes
decreased (p<0.001). There was a higher chance for a more accurate aCTV
coverage of LNs (>90% of the LN volume covered by aCTV) if the LNs were in
the inguinal region as compared to other regions (odds ratio=7.23; 95%-CI [1.09;48.05]) (p=0.041).
Conclusion
ABS with 40 datasets in the ABS-template is a useful tool to delineate CTVs
in patients with anal cancer. However, supervision and correction of ABS-based delineated
volumes by an experienced radiation oncologist is still strongly recommended.