Background and Rationale: MRI
based 3D-IGABT has become an advanced standard for cervical cancer brachytherapy (BT)
and has shown improved clinical outocmes (local/pelvic control, survival, morbidity).
Although MRI is regarded as « gold standard » for IGABT, its
wide applicability is limited by its availability, logistics and financial
implications. Hence, use of CT and UltraSound (US) has been explored. In order to arrive
at a systematic, uniform and international approach for CT based definition and
contouring of target structures, GEC ESTRO, IBS and
ABS agreed to jointly develop such recommendations. They are based on the
concepts and terms as published in the ICRU report 89, defining the advanced standard
approach with repetitive clinical examination at diagnosis (DG) and at BT with
3D documentation and with MRI at DG (MRDG) and at BT (MRBT)
with the applicator in place. The following recommendations
represent a first draft designed by the two first authors.
Development of CT based Recommendations: The minimum
requirements for CT based contouring are clinical examinationDG,BT with
3D documentation and CTDG and
CT with applicator in place (CTBT).
The recommendations are based on GTV and CTV assessment (clin exam, US, MRI), on classification of clinical
remission patterns within various clinico-radiological scenarios.
1. Assessment
of GTV and CTVHR: The cornerstone for CT based target contouring is the repetitive
clinical examination with a revised scaled diagram for documentation. The
CTVHR definition focusses on dimensions related to width, height and
thickness. For width the new “Near Maximum Distance” (NMD) is introduced which
is related to the cervical canal (os) and specified for each parametrium (left,
right). The different volumetric imaging methods (MRI, CT, US,
TRUS) are outlined with emphasis on strengths & limitations. Protocols for CT and US (TRUS) are
suggested to define appropriately anatomical structures for contouring in the various
imaging environments.
Uncertainties are associated with
assessment of GTV at diagnosis (major for CT) and of GTV response (least with
MRI). These uncertainties can be reduced by repetitive clinical examination and
TRUS, beside MRI.
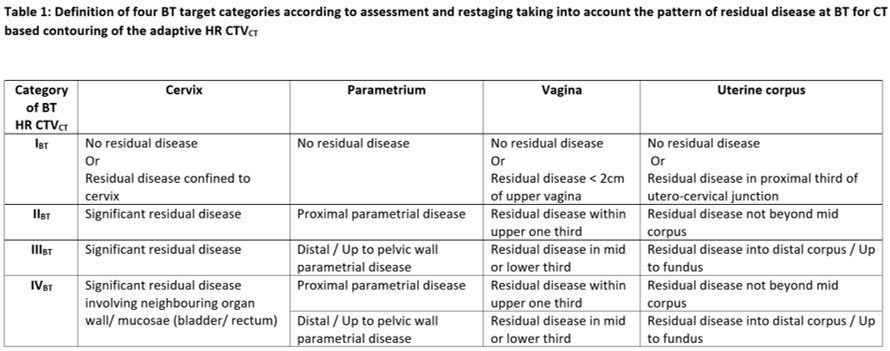
2. Classification of
Clinical Remission:
A classification of common clinical remission patterns is introduced (« restaging »)
related to anatomical structures which are reproducible both on CT and on other
assessment methods (clinical, MRI, US). For the CTVHR definition 4
categories are defined (IBT-IIBT-IIIBT-IVBT)
for the cervix, parametrium, vagina and uterine corpus (Table 1).
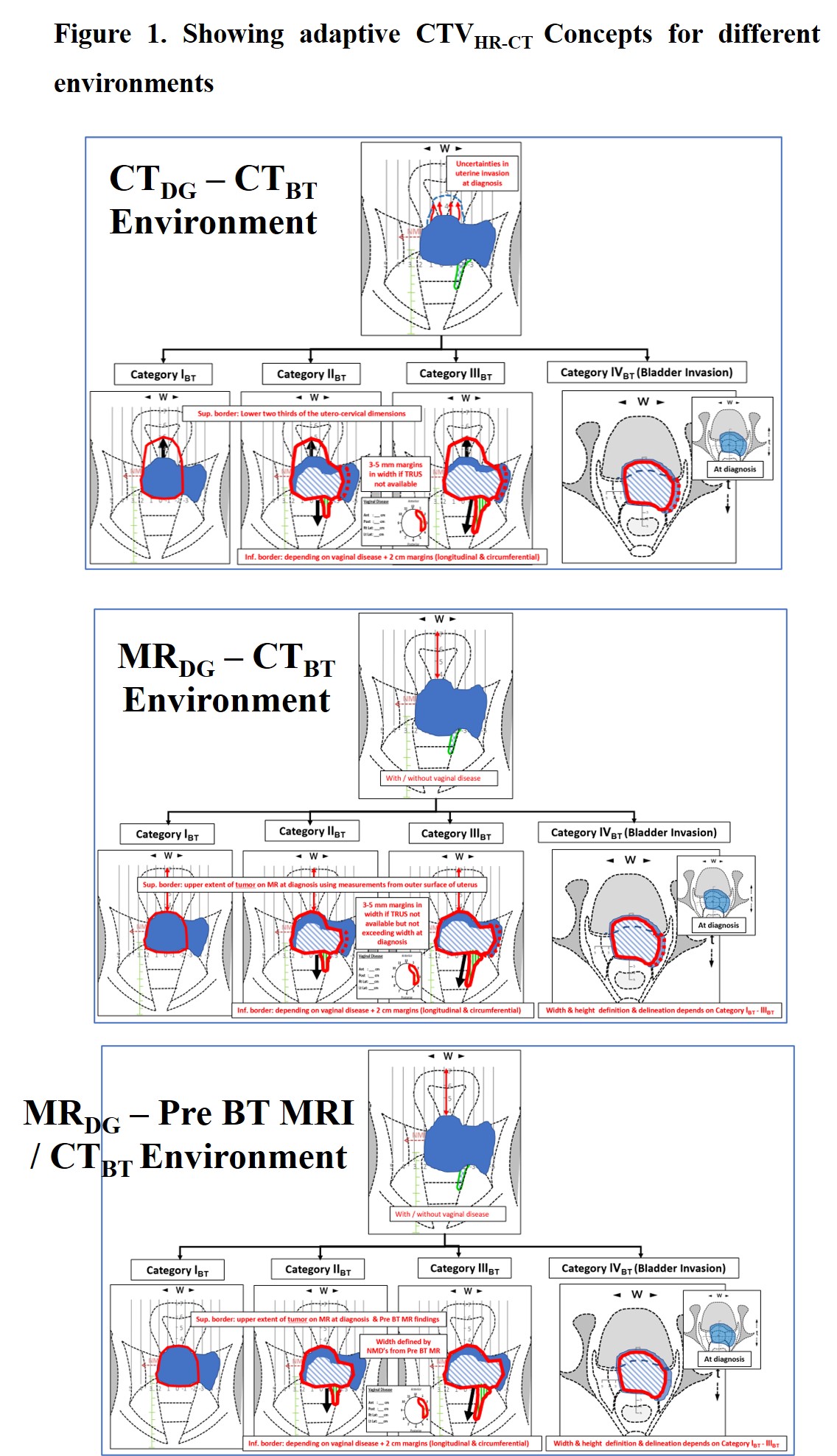
3. Definition of different
clinico-radiological environments: Based on the availaibility of imaging modalities at DG and at BT these
environments are classified into 3 major categories: CTDG
– CTBT ; MRDG – CTBT ; MRIDG
– Pre BT MRI/CTBT. Each environmenrt is divided into 2
sub-categories - with or without real time TRUS - depending on the use
of real time trans-rectal ultrasonography during BT application (6 categories).
4. CT contouring recommendations for definiton and delineation of CTVHR
and OAR: CT based contouring recommendations
were formulated in general for width, height and thickness of CTVHR
and elaborated in detail for the 4 categories of remission pattern
classification related to cervix, parametrium, vagina, and uterine corpus for
the 3x2 clinico-radiological environments (Figure. 1).
For CTDG – CTBT , GTVCT
contouring at BT imaging is not recommended, but is supported for the other
environments. The definition of width,
height and thickness of CTVHR on CT imaging is mandatory for all environments, but represents a
challenge and accounts for major uncertainties and inter-observer variations,
in particular in CTDG – CTBT . These shortcomings
can be minimized through repetitive clin exam with clinical documentation and
more valid and reliable volumetric imagingDG/BT (TRUS, MRI), all
classifying systematically the clinical remission patterns.
For
CT based OAR contouring, a reproducible organ filling status, preferably empty,
and defined protocols of contrast within the organs are vital, especially for bladder
and recto-sigmoid. The major OAR’s are rectum, bladder, sigmoid and bowel.
Discussion:
For each clinico-radiological environment there is an attempt to minimize the
specific uncertainties in order to arrive at the best possible contouring
accuracy. CT based target (OAR) contouring recommendations based on 4 remission
categories within 6 defined environments aim at improving the contouring accuracy
for IGABT using CT, US MRI as available. They will be further discussed in
international expert rounds during the next months and then decided through
IBS, GEC ESTRO (ACROP), ABS before publication.
Evaluating feasibility and reproducibility of these
recommendations and further clinical research on clinical outcome for CT Based
IGABT following these recommendations will become the next steps.