Dysphagia and treatment prolongation due to CRT for upper aerodigestive tract malignancies
PO-1225
Abstract
Dysphagia and treatment prolongation due to CRT for upper aerodigestive tract malignancies
Authors: Petros Alexidis1, Efstathios Kamperis1, Vasileios Giannouzakos1, Maria Topalidou2, Georgios Mpallas2, Vaia Mentesidou2, Ourania Kimoundri2, Chionia Kodona2, Konstantinos Chatzioannou2
1General Hospital Papageorgiou, Radiation Therapy, Thessaloniki, Greece; 2General Hospital Papageorgiou, Radiation Therapy , Thessaloniki, Greece
Show Affiliations
Hide Affiliations
Purpose or Objective
To investigate factors resulting to dysphagia (primary outcome) and treatment delays (secondary outcome) in patients receiving concurrent radiation therapy and chemotherapy for malignancies arising from the oral cavity or oropharynx.
Material and Methods
Retrospective analysis of the patient records who received RT to the primary and bilateral neck lymph nodes concurrently with chemotherapy, was carried out. Logistic regression models were used to investigate predictive factors of dysphagia grade ≥ 2 or prolongation of total treatment duration ≥ 7 days.
Results
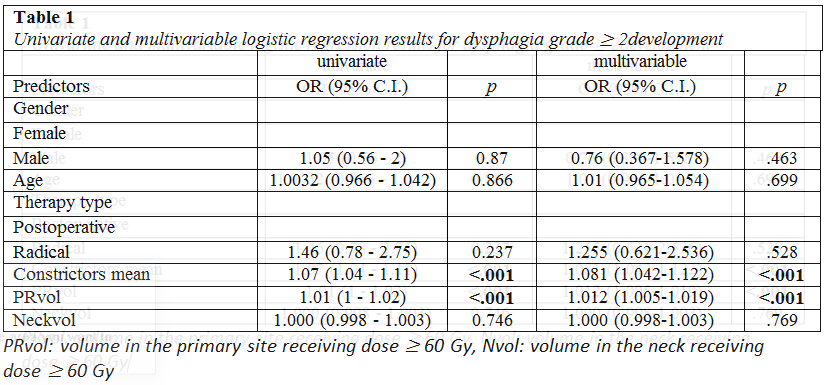
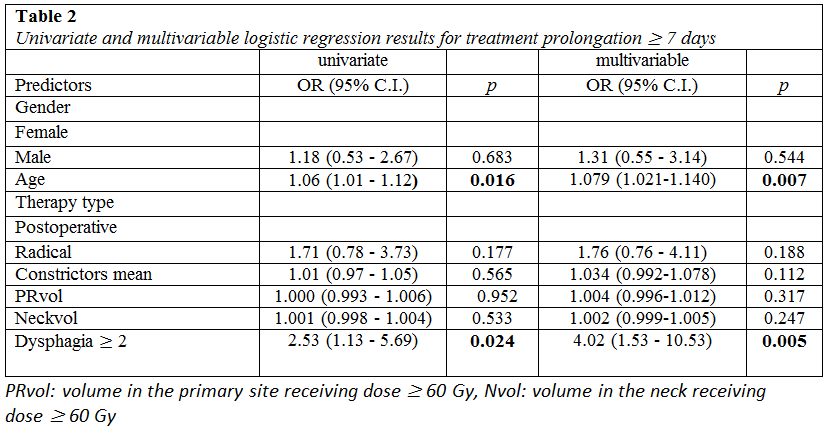
160 patients were included in the study. Mean age was 63.31 (SD= 8.24). The mean treatment duration was 6,7 weeks. 76 (47.5%) developed dysphagia grade ≥ 2, and 32 (20%) experienced treatment prolongation ≥ 7 days. The analysis showed that dysphagia grade ≥ 2 was associated with mean dose to the constrictor muscles > 40.6 Gy (p<0.001, OR = 11.58, 95% CI [4.84 – 27.71]) and to the anatomical volume in the primary that received ≥ 60 Gy (≥ 118.75 cc, p<0.001, (OR = 8.43, 95% CI [3.51 – 20.26]). Elderly patients (p=0.007, OR=1.079, 95% CI [1.021-1.140]) or those that developed dysphagia grade ≥ 2 (p=0.005, OR=4.02, 95% CI [1.53-10.53]) were more likely to experience treatment prolongation ≥ 7 days.
Conclusion
In patients receiving bilateral neck irradiation concurrently with chemotherapy for oral cavity or oropharyngeal cancer, constrictors mean dose and the volume in the primary site receiving ≥ 60 Gy should be kept below 40.6 Gy and 118.75 cc respectively whenever possible. Patients that are more likely to experience treatment prolongation ≥ 7 days are elderly patients or those that are considered at high risk for dysphagia. Close monitoring during the course of treatment for nutritional support and pain management is of great significance.