Hypofractionated re-irradiation for locoregionally recurrent head and neck cancer
Carlotta Becherini,
Italy
PO-1184
Abstract
Hypofractionated re-irradiation for locoregionally recurrent head and neck cancer
Authors: Carlotta Becherini1, Chiara Mattioli1, Niccolò Bertini1, Viola Salvestrini2, Ilaria Bonaparte1, Isacco Desideri1, Vanessa Di Cataldo1, Mauro Loi1, Beatrice Bettazzi1, Luisa Caprara1, Monica Mangoni1, Lorenzo Livi1, Pierluigi Bonomo1
1AOU Careggi - University of Florence, Radiotherapy Unit, Florence, Italy; 2Istituto Fiorentino di Cura e Assistenza (IFCA), CyberKnife Center, Florence, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Loco-regional recurrence is the predominant pattern of failure in patients affected by locally-advanced head and neck cancer (HNC). In both squamous cell carcinoma (SCC) and non-squamous histotypes, there is sparse evidence on the role of photon-based re (RE) irradiation (RT) in this setting. In the context of hypofractionation, different regimens have been adopted in previous experiences. The aim of our single-centre study is to evaluate the clinical outcome of recurrent, unresectable, HNC patients treated with hypofractionated Re-RT.
Material and Methods
We retrospectively reviewed data from 53 consecutive patients with recurrent HNC treated at our centre with 2 courses of RT. All patients were deemed eligible for ReRT for a recurrent, previously irradiated unresectable HNC, following a multidisciplinary discussion of each case. Local control and survival were calculated using the Kaplan-Meier method and log rank test with time measured from the date of last day of Re-RT to date of progression or death.
Results
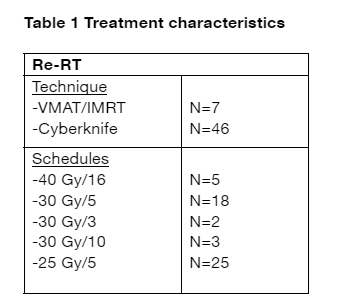
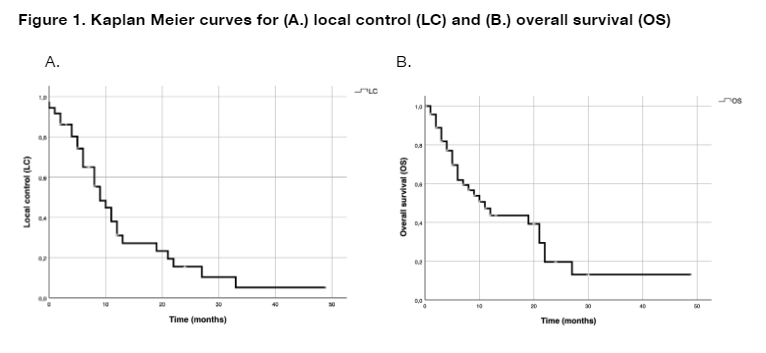
First curatively-intended course of RT was delivered from 1997 to 2020 with or without chemotherapy. Forty patients (75%) had a diagnosis of SCC, while 11 (21%) had other histotypes than SCC; for 2 (4%) patients, histotype was not available. Re-RT was performed from 2012 to 2022 adopting a hypofractionated schedule. Details of Re-RT are shown in table 1. After a median follow-up of 22 months (range 0-49), 24 out of 53 patients were alive. Fourteen patients died for HNC disease (26%), 2 for toxicities related to treatments (4%) while 13 for other causes (24%). The median age of the cohort was 60 years. The median local control (LC) and the 1-year LC rate were 9 months (95% CI 5,6-12,3 months) and 74.2%, respectively. The median overall survival (OS) after re-RT and the 1-year OS rate were 11 months (95% CI 6.0-15.9) and 88,8% (Figure 1), respectively. At univariate analysis, a borderline negative association between time to Re-RT ≤ 12 months and LC was shown (p 0.06). No statistically significant correlation was observed in respect with age ≤ or > 70 years (p 0.19) or gender (p 0.15). A significant dependence of outcome after Re-RT from the hypofractionated schedule could not be demonstrated from our data (p 0.06).
Conclusion
In our experience, multiple hypofractionated Re-RT schedules were shown to be a well tolerated treatment option for HNC recurrence with potential for prolonged local control in appropriately selected patients.