Lexicographic optimization-based planning for brain metastasis radiosurgery with coplanar arcs
PO-1630
Abstract
Lexicographic optimization-based planning for brain metastasis radiosurgery with coplanar arcs
Authors: Sara Trivellato1, Paolo Caricato1, Roberto Pellegrini2, Martina Daniotti1, Gianluca Montanari1, Denis Panizza1, Valeria Faccenda1, Stefano Arcangeli3, Elena De Ponti1
1ASST Monza, Medical Physics Department, Monza, Italy; 2Elekta AB, Medical Affairs, Stockholm, Sweden; 3University of Milan Bicocca, School of Medicine and Surgery, Milano, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
In this study, a not yet commercially available fully-automated lexicographic optimization (LO) planning system, called mCycle (Elekta AB, Stockholm), was validated for intracranial stereotactic radiosurgery (SRS).
Material and Methods
Forty-four consecutive SRS treatment plans (21 Gy/1 fx) delivered between November 2019 and August 2022 were retrospectively selected and automatically re-planned by mCycle (Monaco research version 5.59.13). Twenty-five of them has 1 lesion, 13 had 2 lesions, 4 had 3 lesions, and 2 had 4 lesions. An a-priori assigned priority list, a so-called Wish List (WL), was used to define the sequential LO: four patient sets (WL tuning set) were necessary to tune each robust WL, for single lesion-plans (SLp) and multiple lesion-plans (MLp). While in manual plans (MP), the arc setup is freely chosen by the planner, the WL was tuned to use 2 coplanar arcs of 140° and 360° for SLp and MLp, respectively. A 0° and 90° collimator rotation was set for counter-clockwise and clockwise arcs, respectively. The fluence optimization is followed by a Monte Carlo calculation (MCc) with a 1 mm-dose grid and 0.5%-statistical uncertainty. A target coverage as high as possible was requested, with at least 80% of the prescription dose covering 99% of the PTV. The main criteria for SLp approval was a brain volume receiving more than 12 Gy less than 10 cm³ (V12Gy<10 cm³). In MLp this criterion can be overcome to get the minimum target coverage. Manual plans (MP) and mCycle plans (mCP) were compared in terms of dose-volume constraints, conformality, and monitor units (MUs). Statistical significance was assessed by performing the Wilcoxon-Mann-Whitney test and plan delivery accuracy was verified by pre-treatment QA.
Results
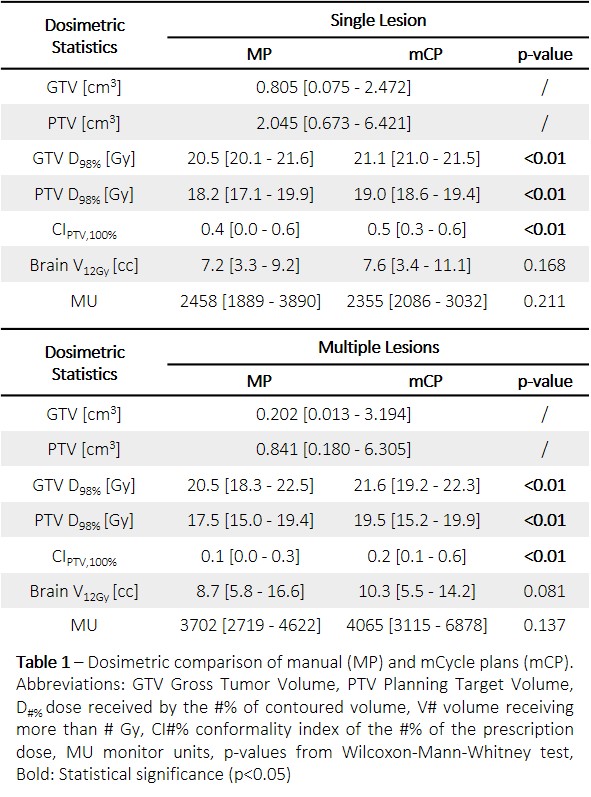
Each WL tuning took 3 days. The median optimization and MCc time can be estimated at 8 hours and 3 hours per MP and mCP, respectively. Results are summarized in Table 1. Statistically significant increases in mCP target coverage and PTV Paddick’s conformity index were registered for both SLp and MLp. Although not statistically significant, mCP showed a higher brain V12Gy. Other organs at risk were never significantly interested by clinically relevant doses. The SL mCP registered a lower median MU number while ML mCP results were obtained with a higher median number of MU. In both cases, this difference was not statistically significant and plans registered a comparable local gamma analysis (2%/2mm).
Conclusion
The novel mCycle autoplanning produced high-quality clinically acceptable radiosurgery SL and ML plans with coplanar arcs, significantly reducing the overall planning time from about one working day for one MP to about 3 hours for one mCP. Together with comparable OAR sparing, the target coverage was significantly increased and preserving the plan deliverability. The validation showed the mCycle capability to generate high-quality deliverable plans according to institutional-specific planning protocols.