Abdominal compression as motion management for stereotactic radiotherapy of ventricular tachycardia?
Annika Mannerberg,
Sweden
PD-0744
Abstract
Abdominal compression as motion management for stereotactic radiotherapy of ventricular tachycardia?
Authors: Annika Mannerberg1, Anneli Edvardsson1,2, Martin P Nilsson2,3, Kristin Karlsson4,5, Sofie Ceberg1
1Medical Radiation Physics, Department of Clinical Sciences Lund, Lund University, Lund, Sweden; 2Department of Hematology, Oncology and Radiation Physics, Skåne University Hospital, Lund, Sweden; 3Division of Oncology and Pathology, Department of Clinical Sciences, Lund University, Lund, Sweden; 4Karolinska University Hospital, Section of Radiotherapy Physics and Engineering, Department of Medical Radiation Physics and Nuclear Medicine, Stockholm, Sweden; 5Karolinska Institutet, Department of Oncology-Pathology, Stockholm, Sweden
Show Affiliations
Hide Affiliations
Purpose or Objective
In recent years stereotactic radiotherapy (RT) for treatment of ventricular tachycardia (VT) has been introduced. Studies have shown that this non-invasive treatment can largely reduce VT episodes (Cuclich et al. 2017, Neuwirth 2019). However, delineation of the target is not straightforward and the final target volume have to include the VT substrate, the associated cardiac and respiratory motion and other uncertainties (Lydiard et al. 2021). The final treatment volume can therefore be large and include healthy heart tissue. A common motion management technique for respiratory motion reduction is to use abdominal compression. However, the benefit of compression for patients with VT undergoing RT has not yet been thoroughly investigated. The aim of this study was therefore to compare the effect of abdominal compression on motion in the heart and surrounding tissues.
Material and Methods
Eight patients were retrospectively enrolled in the study. Two 10 phase four dimensional computed tomography (4DCT) were acquired for each patient, one with abdominal compression and one without. The left coronary artery, the left anterior descending artery (LAD), the lateral wall of the left ventricle and the apex were delineated in the heart. Additionally, the carina, the right and left diaphragm cupola were delineated. Structures were delineated in the maximum expiration and maximum inspiration phase respectively in both 4DCT data sets. Maximum expiration and inspiration phase were defined as the phase with smallest and largest total lung volume respectively. The LAD, left coronary artery, carina, left and right diaphragm were delineated as small point structures. The apex was delineated at the two most caudal slices of the heart and the left ventricle wall was delineated as the 1 cm most lateral part from cranial slice to apex. The center of mass (CoM) distance from expiration to inspiration phase was compared between with and without compression for each structure. For statistical analysis the Wilcoxon signed-rank test with a significance level of 0.05 was used.
Results
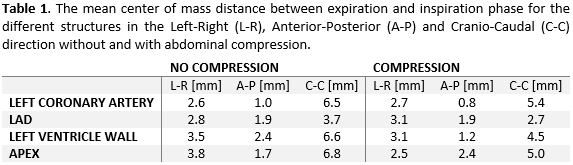
For the mean CoM dictance, only small differences between with and without compression were observed, none of which were statistically significant (Table 1). For some patients and structures the motion of CoM increased when using compression (Figure1). Statistically significant difference was observed for the right diaphragm cupola in the Cranio-Caudal (C-C) direction (p=0.02) and the left diaphragm cupola in anterior-posterior (A-P) direction (p=0.03), indicating that the abdominal compression plate was placed correctly on the patient.

Conclusion
Respiratory associated motion of the heart did not statistically significantly decrease when abdominal compression was used, indicating that the benefit of compression for VT patients receiving RT is limited. Future work involves further investigation of the optimal motion management for these patients, including dosimetric evaluation of abdominal compression and exhale/inhale breath hold RT.