Online adaptive CBCT-guided VMAT radiotherapy using an Elekta Synergy CBCT-linac
Maureen Groot Koerkamp,
The Netherlands
PO-1940
Abstract
Online adaptive CBCT-guided VMAT radiotherapy using an Elekta Synergy CBCT-linac
Authors: Maureen Groot Koerkamp1, Gijsbert Bol1, Petra Kroon1, Annick Scheeren1, Annelies Zoetelief1, Lean Krikke1, Tessa Harderwijk1, Annika Plat1, Stefan van der Vegt1, Jochem Hes1, Ineke van Gasteren1, Geja Schimmel-de Kogel1, Esmee Renders1, Joost van Kaam1, Roos Onnink-Vijfvinkel1, Dennis Winkel1, Mike van Rijssel1, André Wopereis1, Juus Noteboom1, Sandrine van de Pol1, Wietse Eppinga1, Jochem van der Voort van Zyp1, Corine van Es1, Jannette Bossenga1, Bas Raaymakers1
1University Medical Center Utrecht, Radiotherapy, Utrecht, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
The aim was to develop and implement a first-in-person daily online adaptive radiotherapy workflow for an Elekta Synergy CBCT-linac. Requirements were to use clinically approved tools and to minimize user interaction.
Material and Methods
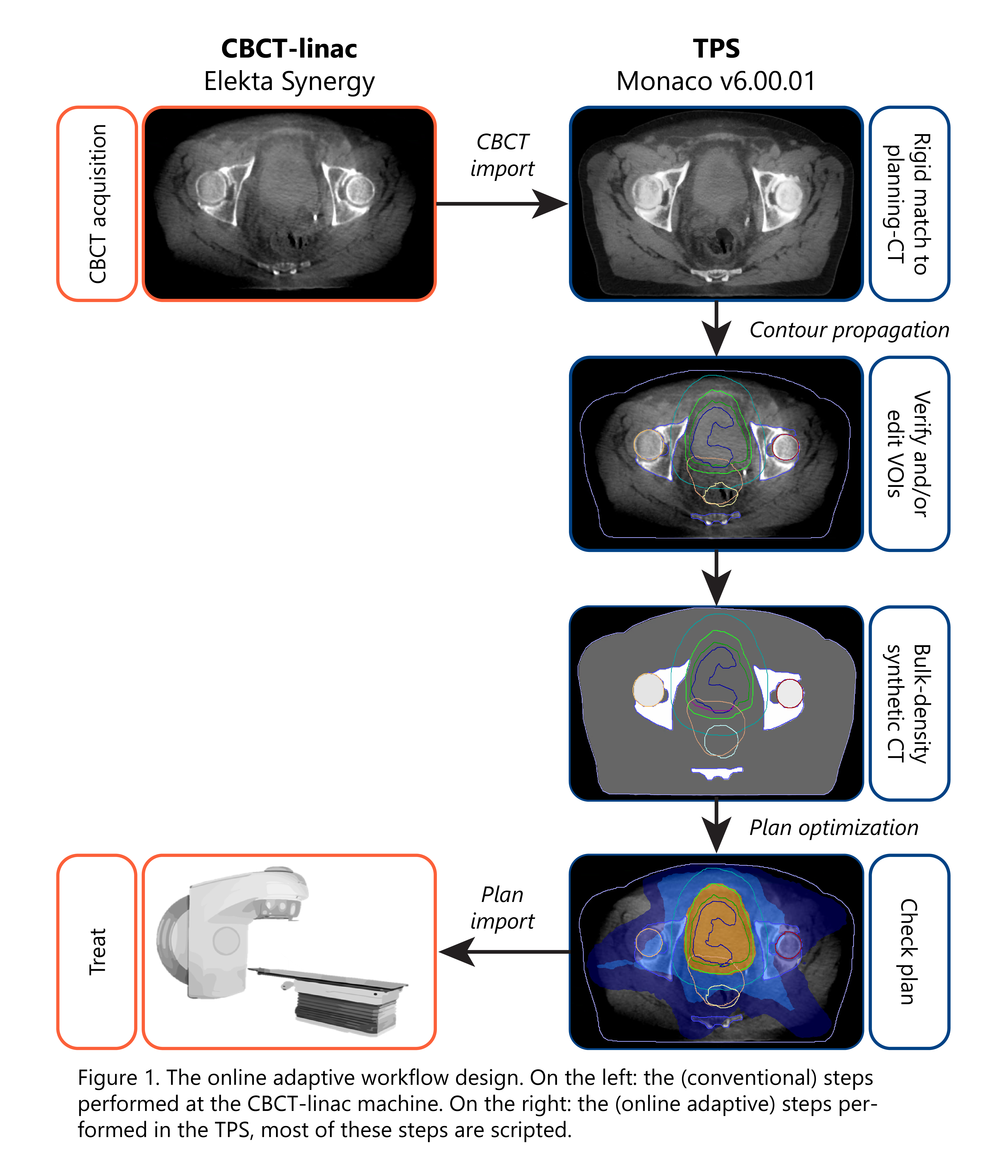
In the proposed workflow, the daily CBCT is used as planning scan and is sent to the treatment planning system (TPS). In the TPS, the following steps take place: contour propagation and bulk-density propagation from planning-CT to CBCT, contour editing, plan optimization (VMAT) and plan verification. If approved, the plan is exported to the treatment delivery software to start treatment delivery.
During workflow development, we evaluated the CBCT image quality, created a planning template, evaluated the workflow duration, performed a risk analysis and implemented measures to minimize risks. Multiple dry runs were performed to test the workflow.
Results
We successfully developed the workflow for treatment of palliative bladder patients (Fig. 1). The TPS part is scripted using Monaco scripting tools. Interaction with the TPS is only required for patient selection, start of CBCT import, contour checking and editing, and plan approval. A VMAT plan is optimized from scratch without user interaction. After export, the online plan is manually entered into the treatment delivery software to start treatment delivery. In-house developed tools are used to send the data between the different systems and to add safety measures to minimize the risks identified.
The current CBCT protocol showed acceptable image quality, when excluding patients with a hip prosthesis. A generic planning template (single 360º VMAT arc) was developed for automated plan optimization. It uses multicriterial optimization to optimize OAR sparing. To accelerate optimization, the calculation grid was reduced from 3x3x3 mm³ to 4x4x4 mm³. Test plans for two fractions in ten retrospective patients showed good target coverage with equal or improved OAR sparing compared to recalculation of the clinical plan. QA measurements of test plans showed good plan quality: mean gamma pass rate 99.5% (3%/3mm).
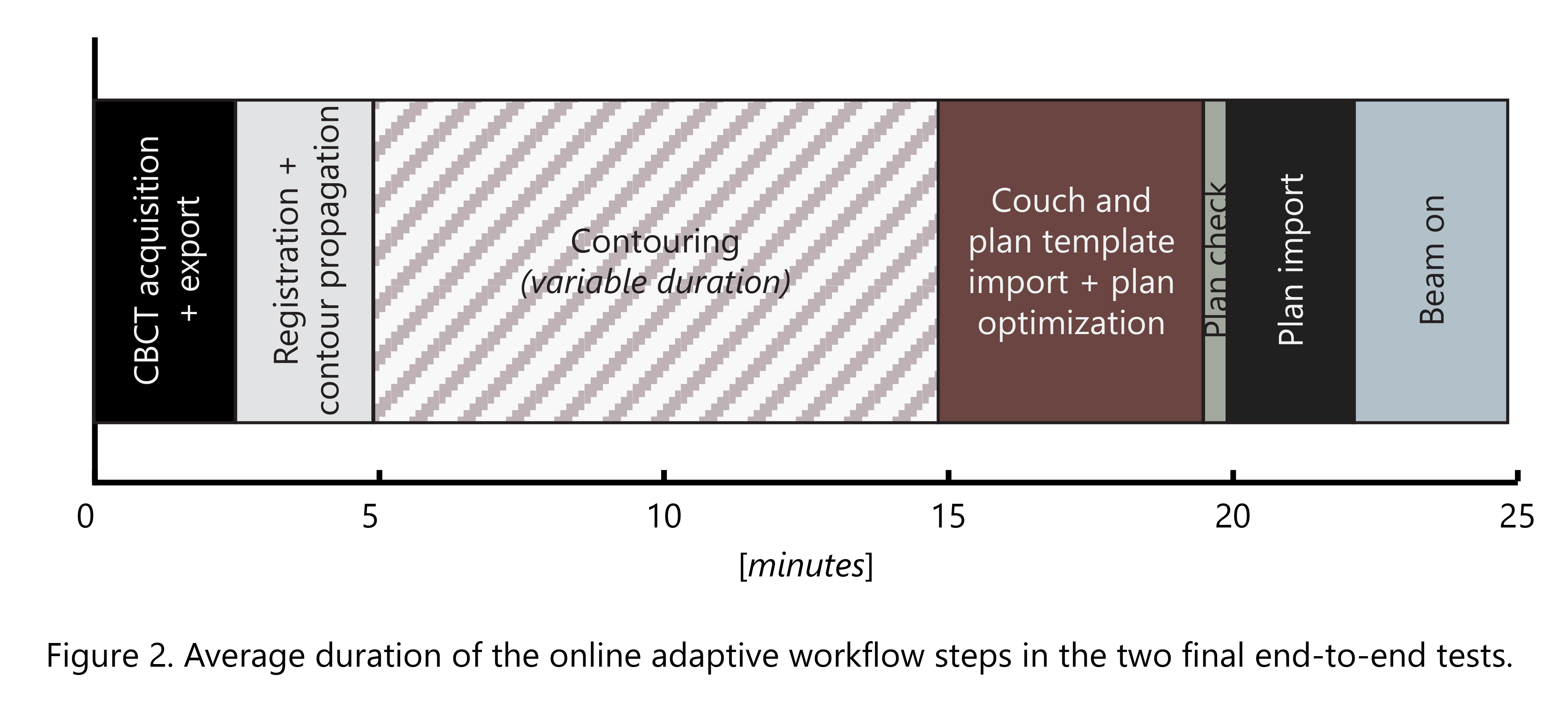
Multiple workflow tests were completed successfully. The average workflow duration is shown in Fig. 2, indicating that with a maximum contouring time of 10 minutes, the workflow length stays below 25 minutes. Average plan optimization time is 3 minutes.
Different disciplines have been trained to perform the workflow. The workflow is RTT-led and supervised by a radiation oncologist. A medical physicist will be present during the first fractions. A pilot was started to show the feasibility of the workflow in three 10/13x3 Gy palliative bladder patients.
Conclusion
We developed and implemented an online adaptive CBCT-guided VMAT workflow for an Elekta Synergy CBCT-linac. As of October 2022, we started a pilot in which the workflow is our clinical procedure.