Feasibility study of the Transit-Guided Radiation Therapy technique: an interim analysis
Artur Latorre-Musoll,
Spain
PO-1928
Abstract
Feasibility study of the Transit-Guided Radiation Therapy technique: an interim analysis
Authors: Artur Latorre-Musoll1, Marta Marín de Castro2, Sergi Serrano2, Gabriela Antelo2, Gabriela Oses2, Meritxell Mollà2
1Hospital Clínic de Barcelona, Servei d'Oncologia Radioteràpica (ICMHO), Barcelona, Spain; 2Hospital Clínic de Barcelona, Servei d'Oncologia Radioteràpica (ICMHO), Barcelona, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
Transit-Guided Radiation Therapy (TGRT) is a promising technique that can provide on-line corrections to position errors by assessing the transit portal images (TPIs) of the treatment fields (Phys Med Biol 2022 67 155022). In this work we present the preliminary results of an ongoing prospective clinical study aimed to assess, for the first time, the performance of the TGRT technique in a clinical setting.
Material and Methods
The TGRT technique uses the TPIs to assess the position error projected to the EPID plane, which is denoted by the shift vector s.
To validate the TGRT technique, breast and whole-brain plans have been used to obtain TPIs from gantry-static fields with skin flash. Such fields directly irradiate a region of the EPID extending beyond the body contour, which defines a sharp edge on the TPIs that can be used as a surrogate of the patient position. An in-house code has been developed to identify the projection of the body contour onto a given TPI by using an edge-detection algorithm. Then, the code rigidly registers the body contours of a given TPI and the first TPI (used as reference), yielding the true shift projected at the EPID plane s_0 between these two fractions of that field. The TGRT-based shifts s have been compared to the edge-based shifts s_0 (which constitutes the gold standard set) for all fields and fractions. A total of 262 TPIs obtained from ten patients treated with 3DCRT have been evaluated in this interim analysis: 6 breasts with breath-hold (202 TPIs), 3 breasts in free-breathing (42 TPIs) and 1 whole-brain (18 TPIs).
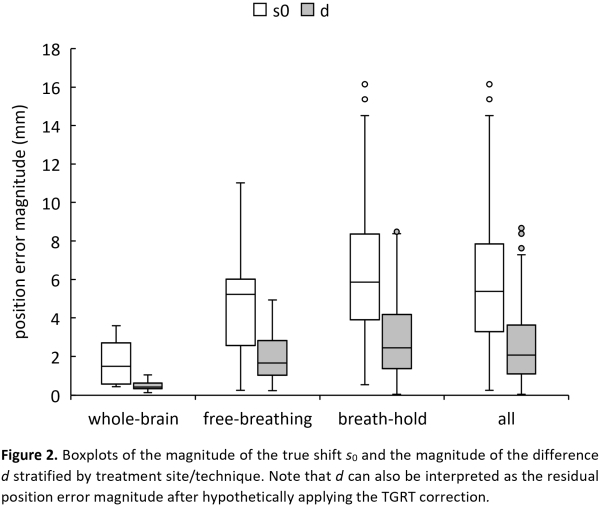
The magnitude of the difference d = |s – s_0| has been obtained for all fields and fractions. The differences d have been compared to the magnitudes of the corresponding true shifts s_0 ≡ |s_0| by using a left-tailed paired-data t-Student test (stratified by site/technique) to check whether the TGRT technique, if applied, could have reduced the existing position error (d < s_0) or not (d ≥ s_0) (significance level α = 0.05).
Results
Figure 1(a) shows a correlation of R2 = 0.76 between the components of the TGRT-based shifts and the edge-based shifts. Figure 1(b) shows that most of the TGRT-based shifts (92%), if applied, would have reduced the existing position error (d < s_0). Most of the overcorrections (18 out of 21) corresponded to small true shifts below 5 mm, i.e., with a minor clinical impact.
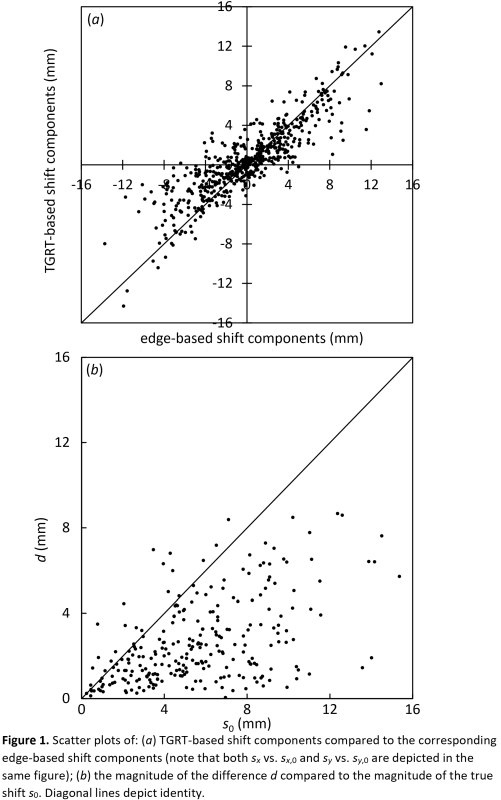
Figure 2 shows that the TGRT technique (if applied) can significantly reduce the existing position error regardless of the treatment site (p = 6E–5 for whole-brain, p = 1.6E–9 for breasts in free breathing, p = 1.0E–38 for breasts in breath-hold and p = 1.1E–47 overall).
Conclusion
The preliminary results of the ongoing clinical study are very promising, suggesting an excellent performance of the TGRT technique in a clinical setting. Validations for additional treatment sites and techniques are work in progress.