Larynx treatment: dose reduction in the carotids and plan robustness
Helena Vivancos Bargalló,
Spain
PO-1915
Abstract
Larynx treatment: dose reduction in the carotids and plan robustness
Authors: Helena Vivancos1, Nuria Jornet1, Jaime Perez-Alija1, Cristina Anson1, Pedro Gallego1, Marta Barcelo1, Natalia Tejedor1, Alex Dominguez1, Nagore Garcia-Apellaniz1, Fatima Leo1, Agusti Ruiz-Martinez1, Pablo Carrasco de Fez1
1Hospital de la Santa Creu i Sant Pau, Medical Physics, Barcelona, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
Modulated treatment techniques have shown a better carotid sparing for larynx EBRT treatments. The aim of this study was to evaluate plan robustness (CTV and PTV coverage and dose to carotids) to inter-fraction rigid and not rigid positioning differences for 7 different EBRT techniques using X-rays.
Material and Methods
10 patients were included in the study. Patients were immobilised using a thermoplastic mask. GTV, CTV, PTV (CTV+5mm) and carotids were delineated. The dose prescription was 2 Gy x 35 fractions. A NAL5 + weekly CBCT was used for most patients. No corrections were applied if the Δ<3mm. For each patient 7 different treatment plans were prepared: 3D and IMRT & VMAT with the following avoidance volumes: none, shoulders (*) and shoulders & chin (**). The plans were optimised in Eclipse TPS to fulfil PTV D98 > 95%. An uncertainty planning study for each of the plans was performed by simulating 5mm rigid movements in the three axes. Then, the dose distribution for each plan was recalculated in Eclipse using the weekly CBCTs. Finally, the results of an in vivo system, using 2D EPID transmission dose and logfile based dose recalculation on the CBCT were compared for the real patient treatment (7 3DCRT; 1 IMRT**; 2VMAT**).
Results
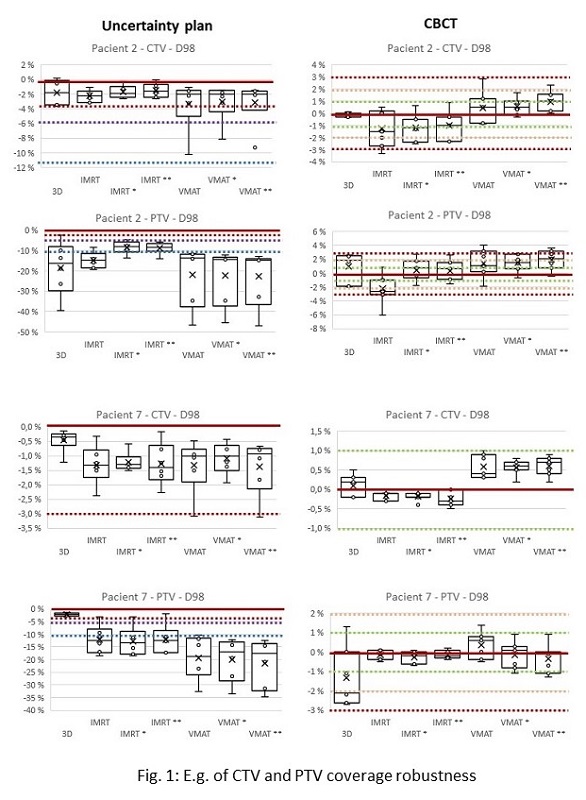
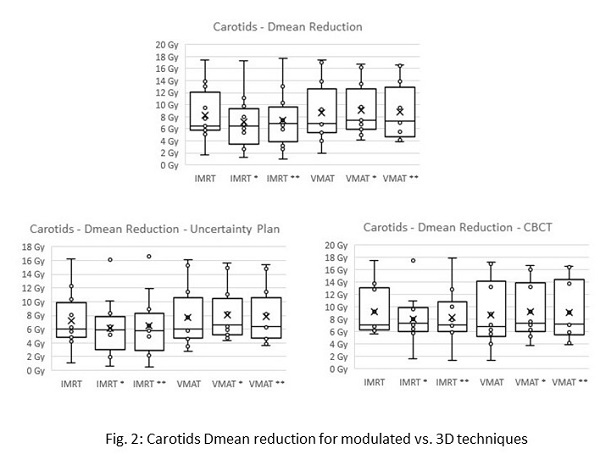
Table 1 shows the results of the uncertainty plan (A) regarding CTV and PTV coverage as the number of patients for whom the resulting dose distribution fulfils a coverage of the CTV and PTV within 3 or 5% with respect to the approved plan. For the CBCT recalculation (B) the number of patients that would fulfil the criteria of CTV and PTV coverage in all the fractions is shown. We found a 90% false positive 2D IVD results for 3DCRT and IMRT** and 50% for VMAT**. The agreement for the CBCT dose recalculation was better than 90% for all treatment fractions and techniques. Results for the CTV and PTV coverage for two different patients are shown in figure 1 as an example. Fig. 2 shows the dose reduction for the different techniques compared to 3DCRT as well as its robustness to changes in patient positioning.
|
| D98%plan ± (x) | 3DCRT | IMRT | IMRT* | IMRT** | VMAT | VMAT* | VMAT* |
| A | CTV | 3% | 7 | 6 | 9 | 10 | 4 | 5 | 4 |
| A | CTV | 5% | 10 | 10 | 10 | 10 | 6 | 7 | 5 |
| A | PTV | 3% | 4 | 1 | 1 | 1 | 0 | 0 | 0 |
| A | PTV | 5% | 7 | 2 | 1 | 1 | 0 | 0 | 0 |
| B | CTV | 1% | 4 | 1 | 2 | 2 | 0 | 2 | 1 |
| B | CTV | 2% | 6 | 3 | 6 | 3 | 4 | 6 | 3 |
| B | PTV | 1% | 1 | 1 | 2 | 1 | 0 | 0 | 0 |
| B | PTV | 2% | 1 | 1 | 2 | 3 | 1 | 2 | 1 |
Table 1
Conclusion
IMRT and VMAT significantly reduce the mean dose to carotids and this difference is robust for the inter-fraction differences.
The uncertainty plan is a poor estimator of patient inter-fraction differences, it doesn’t account for non-rigid movements.
Robustness is better for 3D (CTV) and IMRT (PTV). It improves when adding the shoulders as an avoidance volume.
2D transit IVD: false positives due to the position of the shoulders at the beam exit. Good estimator of inter-fraction positioning differences , useful to flag patients that need daily imaging.
3D dose recalculation (logfiles and CBCT): good estimator even if sometimes differs from Eclipse recalculation due to differences in the body contour and dose calculation algorithms.