Liver deformability as residual error in stereotactic radiotherapy of hepatic metastases
PO-1912
Abstract
Liver deformability as residual error in stereotactic radiotherapy of hepatic metastases
Authors: Valeria Panni1, Elena Galofaro1, Clelia Di Carlo1, Mohamed Vincenzo Agbaje Olufemi1, Francesco Fenu1, Lisa Vicenzi1, Lucio Alticozzi2, Francesca Cucciarelli1, Marco Valenti2, Giovanna Mantello1
1Azienda Ospedaliero Universitaria delle Marche, Radiotherapy Department, Ancona, Italy; 2Azienda Ospedaliero Universitaria delle Marche, Medical Physics, Ancona, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
In liver stereotactic radiotherapy (SRT), breath control methods and image-guided radiotherapy (IGRT) are recommended techniques to online correct the uncertainties that characterize this treatment. Liver deformability is a liver feature, mainly influenced by neighboring OARs filling and position, that represents an important issue in the setting of liver SRT, since it is not online correctable by IGRT. Aim of this study was to assess and offline quantify liver deformability as residual error after online IGRT match in patients treated with liver SRT in our Department.
Material and Methods
The CBCTs from a sample of 8 patients with liver metastases were analyzed. CT simulation was performed with abdominal compression for 1 patient and breath hold (BH) for 7 patients. The radiotherapy treatment was provided through 3 or 5 fractions. Whole liver silhouette was offline delineated on each daily CBCT (acquired in BH in 7 out of 8 patients) and compared to liver contour on planning CT. On the basis of liver/liver match between CT planning and each daily CBCT, liver center of mass shift on 3 axes (x, y and z) was calculated. Dice Similarity Coefficient (DSC), as deformability index, was estimated.
Results
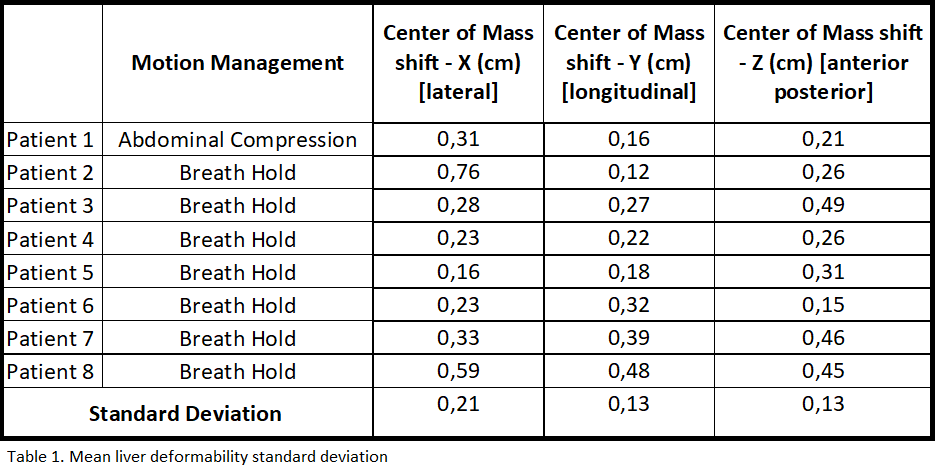
Breath hold technique was well tolerated and reproduced. Liver deformability was analyzed for all the sample. The standard deviation for the center of mass shift was evaluated for the 3 axes in all the patients, as shown in Table 1. According to the results, the liver deformability is bigger in the – X axe, probably due to the interfraction filling variation of the abdominal hollow organs (stomach, bowel). This was considered as a preliminary result of interfraction Internal Margin (IM) to extend PTV margin. The mean DSC was 0.87.
Conclusion
Our results demonstrated that, although breath hold technique for liver SRT resulted an effective technique, with a residual organ motion <= 5 mm, liver deformability represented a residual error that is not online correctable, to consider also in breath hold patients. Deformability was offline quantified for all patients and considered as IM for the PTV definition, with an additional margin of 2 mm. Considering the possible positions of liver metastases, it will be interesting also to evaluate the partial deformability of the liver, related to the location of the lesion.