The role of in vivo dosimetry in the continuous quality improvement of lung stereotactic treatments
PO-1736
Abstract
The role of in vivo dosimetry in the continuous quality improvement of lung stereotactic treatments
Authors: Marco Esposito1, Pietro Mancosu2, Andrea Bruschi3, Alessandro Ghirelli4, Silvia Pini4, Paolo Alpi5, Raffaella Barca4, Camilla Delli Paoli5, Fiammetta Meacci5, Barbara Grilli Leonulli5, Simona Fondelli5, Lisa Paoletti5, Silvia Scoccianti5, Serenella Russo5
1Azienda Sanitaria ULS Toscana Centro, Medical Physics, Firenze, Italy; 2Humanitas Clinical and Research Hospital, Medical Physics, Rozzano, Italy; 3Azienda Sanitaria USL Toscana Centro, S. C. Fisica Sanitaria, Firenze , Italy; 4Azienda Sanitaria USL Toscana Centro, S. C. Fisica Sanitaria, Firenze, Italy; 5Azienda Sanitaria USL Toscana Centro, S. C. Radioterapia, Firenze, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
In this work we reported our experience in the use of in vivo dosimetry (IVD) to improve the dosimetric accuracy of lung stereotactic treatments.
Material and Methods
A commercial software, based on the Electronic Portal Imaging Device (EPID) signal, was used to reconstruct the actual dose of lung stereotactic treatments. The tolerance level was set at 5% PTV mean dose difference or 10% PTV minimum and maximum dose difference.The study was designed in two-phases: an obstervatory and an active phase. In the observational phase, the IVD results of 41 consecutive patients were retrospectively reviewed and out of tolerance cases (OTL) were studied by a multidisciplinary team including a medical physicist, a radiation oncologist and a radiotherapy technician for root cause analysis. The OTL were further divided in deviations beyond safe and acceptable limit, correction required, and deviations not requiring corrections. In the active, prospective phase, the IVD results of 52 patients were analyzed just after the fraction end, and corrective actions were taken when needed. Moreover, proactive preventions were further introduced to reduce the risk of future failures. The error occurrence rate was analyzed to evaluate the effectiveness of proactive actions.
Results
A total of 330 fractions have been analyzed. Considering all fractions analyzed in both phases, the average PTV differences were (-1.1 ± 3.8) %, (3.8% ± 7.3) % and (-0.7 ± 3.9) % for mean, minimum and maximum doses, respectively (FIG1). In the ipsilateral lung the average mean dose difference was (0.9 ± 8.5) %. In the first phase 13 errors have been identified. In the active phase, 12 errors were detected, 5 of which needed corrective actions; in 4 patients the actions taken corrected the error. Several preventions and barriers have been introduced to reduce the risk of future failures: the planning checklist was updated; the procedure for vacuum pillows was improved; and the use of the respiratory compression belt was optimized. A decrease of the failures rate was observed, showing the effectiveness of procedural adjustment.
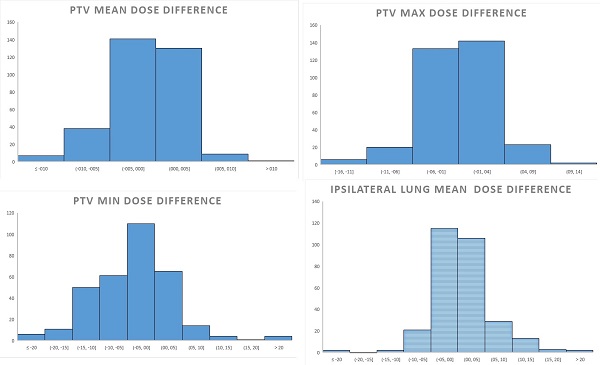
Fig1 Histogram of dose differences in PTV and in the ipsilaterl lung for all the analyzed 330 fractions.
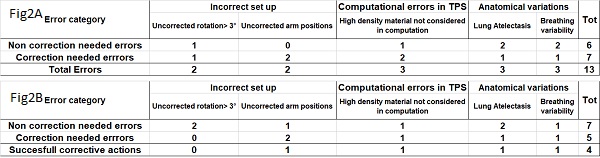
Fig2. Errors found and corrective actions taken in the first Observational phase (Fig2A), and in the second Active phase (Fig2B).
Conclusion
The use of IVD allowed to improve the quality of lung SBRT treatments. Patient specific and procedural corrective actions were successfully taken, leading to an overall improvement of the dosimetric accuracy.