Logfile based automatic patient QA for daily MR guided adaptive radiotherapy
PO-1730
Abstract
Logfile based automatic patient QA for daily MR guided adaptive radiotherapy
Authors: David Tilly1,2, Samuel Fransson2,3, Martin Lundmark4, Ulf Isacsson2,5, Adam Johansson2,6,3
1Uppsala University, Immunology, Genetics and pathology, Uppsala, Sweden; 2Uppsala University Hospital, Medical Physics, Uppsala, Sweden; 3Uppsala University, Radiology and Surgery, Uppsala, Sweden; 4Uppsala University Hospital, Medical Physics, Uppsala University, Sweden; 5Uppsala University, Immunology, Genetics and Pathology, Uppsala, Sweden; 6Uppsala University, Immunology, Genetics and Pathology, Uppsala, Sweden
Show Affiliations
Hide Affiliations
Purpose or Objective
Patient QA for daily adaptive radiotherapy with the MR-Linac requires new methods compared to conventional radiotherapy as the plan cannot be measured using a phantom prior to delivery. Currently the daily plan is measured using a phantom after delivery to assess if any corrective measures are necessary. However, measuring every adapted plan is very time consuming. Therefore, we have implemented an alternative automatic QA workflow based on logfiles from the MR-Linac.
The current work reports on the result of the logfile analysis based on the 226 latest fractions delivered on the MR-Linac.
Material and Methods
The analysis compares a logfile from the daily specific fraction with the Dicom treatment plan created online for that same fraction. The online plan is exported to a local Dicom server and in-house software automatically identifies the corresponding logfile and proceeds with the comparison. The result is easily inspected in a result file produced by the software.
The logfiles contains the complete information of the collimating elements, i.e. the position of each individual MLC leaf as well as jaw, together with the delivered MU at a frequency of 25 Hz.
The comparison criteria used in our institution when comparing the logfile vs the plan are,
• Position of each Jaw and every individual MLC leaf (max error < 1 mm, mean error < 0.5 mm)
• Total delivered MU (error < 2% of treatment plan MU)
• Gantry angle (error < 0.5 degrees)
• Monitor unit maps (MU maps) per beam (max error < 2% compared to total plan MU)
All plans were also delivered on a Delta4 phantom and evaluated with the gamma criteria 3%/3mm vs the dose calculated in the TPS.
Results
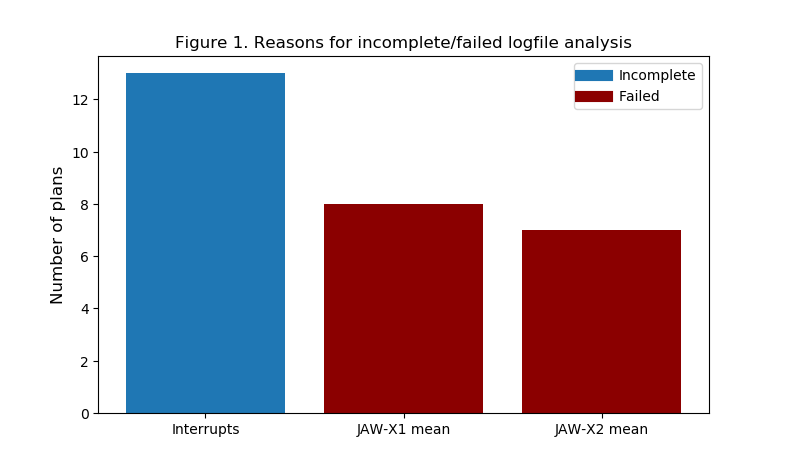
The logfile analysis produced a result in 224 of the 226 fractions. In 90.2% of the 224 logfiles all test criteria passed. The frequency of reasons for logfile not passing the patient QA can be seen in figure 1. In 13 of the failed 22 plans (6% of all plans) the cause was an interrupted treatment which produces multiple logfiles which broke the automatic workflow. In most of the 9 plans with Jaw mean position failure both Jaws failed and are counted twice in Figure 1. The errors in the Jaw mean position did not result in an error in the MU map comparison.
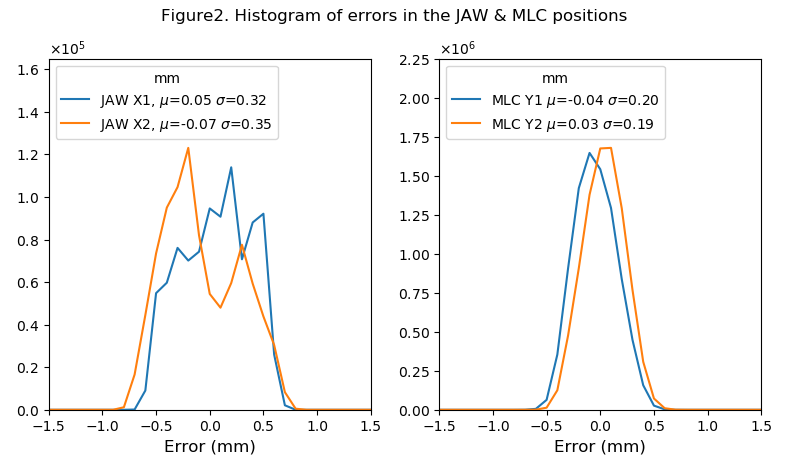
The combined distribution, from all fractions without delivery interruptions, of errors in the positioning of the Jaw and MLC according to the machine logfiles can be seen in figure 2. The mean is very close to 0 mm which means that no systematic errors could be found.
Not a single plan failed the Delta4 measurement criteria, so the errors found in the logfile analysis did not translate into errors in the phantom measurement.
Conclusion
An automatic method for patient QA was implemented and evaluated for > 200 fractions on the MR-Linac. The patient QA was able to evaluate 99% of the fractions and reported that 90.2% of all fractions were delivered according to plan. The logfile analysis was incomplete in 6% of all plans due to treatment interruption.