Total Body Irradiation (TBI) for hematopoietic stem cell transplantation
URIEL ALEXANDER CORRO VERDE,
Spain
PO-1166
Abstract
Total Body Irradiation (TBI) for hematopoietic stem cell transplantation
Authors: URIEL ALEXANDER CORRO VERDE1, Uriel Alexander Corro Verde2, Cristina De La Fuente Alonso2, Jesús Romero Fernandez2, Marta López Valcárcel3, Beatriz Gil Haro2, Joaquin Velasco Jimenez2, Raquel Benlloch Rodriguez2, Sofia Santana Jimenez2, Lucia Paisán Palacio2, Rosario Rubiato Aragon2, Alfonso Valcárcel Diaz2, Patricia Sarrión Rubio de la Torre2, Olga Engel2, Jorge Fernando Obeso Herrera2, Irma Zapata Paz2, Maria Hernández Miguel2, Sofia Cordoba Largo2
1Hospital Universitario Marqués de Valdecilla, Serivicio de oncología radioterápica, Santander, Spain; 2Hospital Universitario Puerta de Hierro, Servicio de oncología radioterápica, Madrid, Spain; 3Hospital Universitario Puerta de Hierro, Servicio de oncología radioterápica, Madrid, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
Total body irradiation (TBI) has been an important component of the conditioning regimen for allogeneic myeloablative hematopoietic stem cell transplantation (HSCT) in acute lymphoblastic leukemia (ALL). The myeloablative conditioning regimen has two aims: (1) to eradicate leukemic cells, and (2) to prevent rejection of the graft. Its use as conditioning regimen for ALL is progressively declining because concerns of toxic effects in favour of chemotherapy-based regimens. This retrospective study aimed to asses that the schedule of 10Gy (2Gy/fraction) give similar results to that reported for classic fractionation (12-15Gy).
Material and Methods
Between 2011-2021, sixty-four patients were treated with TBI conditioning regimen with myeloablative intention. Most patients had a diagnosis of ALL (52/64patients). Fifty-eight patients received 10Gy (90.6%); 12Gy (4.7%), 6Gy (3.1%) and 4Gy (1.6%) in 2Gy per fraction/twice/daily. Patients were positioned in lateral decubitus with lung shielding to limit the average lung dose to 8Gy. In vivo dosimetry was used in all patients. Fifty-six percent achieved complete response with first chemotherapy line before TBI. Forty-four percent needed multiples induction regimens of chemotherapy to achieve response before receiving TBI. The donors were as follow: HLA-matched sibling donor (50.3%), unrelated donor (20%), umbilical cord blood (28.1%) and one case (1.6%) haploidentical transplant.
Results
Mean follow-up: 35 months (range 0-136). Mean overall survival (OS): 42.4 weeks (CI95: 29.2-55.6). One and 2-years overall survival (OS) were 58% and 35%, respectively. Recurrent disease was observed in 17 patients. The median disease-free survival was 7.1months (CI95: 3.4-11.1). Acute side effects are described in Table 1.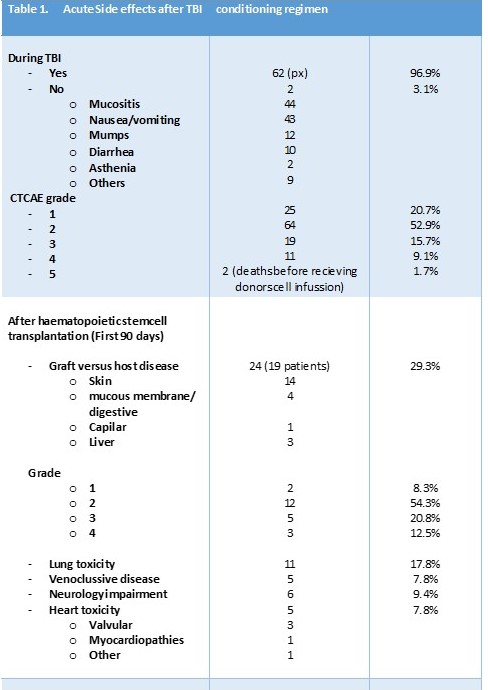
Conclusion
Despite the sample limitation, we can concluded that 10Gy fractionation has similar OS than higher dose schedules with acceptable tolerance.