Hypofractionated and Intensified Radiotherapy for nonsurgical Glioblastoma Multiforme
Íñigo Nieto Regueira,
Spain
PO-1147
Abstract
Hypofractionated and Intensified Radiotherapy for nonsurgical Glioblastoma Multiforme
Authors: Íñigo Nieto Regueira1, Beatriz Vázquez Barreiro2, Virginia Ochagavia Galilea1, Victor Muñoz Garzón1
1Hospital Meixoeiro. Complejo Hospitalario Universitario de Vigo, Radiation Oncology, Vigo, Spain; 2Hospital Meixoeiro. Complejo Hospitalario Universitario de Vigo, Radiation Oncology , Vigo, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
INTRODUCTION
Glioblastoma Multiforme (GM) still has a poor prognosis. The association of surgery , adjuvant Radiotherapy and concurrent Temozolomide is the standard treatment. The median overall survival, is 14.6 months according to Stupp trial.
If the predicted postoperative morbidity and mortality are high, surgery is contraindicated. and Radiotherapy is then, the first treatment option. In these cases of biopsied patients, overall survival is considerably reduced. Conventional RT dose is 60 Gy total dose, 2 Gy per day.
Our porpuse es to analize the tolerance and overall survival(OS) in patients with nonsurgical Glioblastoma Multiforme, (biopsied patients) treated with Hypofractionated and Intensified Radiotherapy (HIRT), in a phase II prospective trial.
Material and Methods
Between January 2016 and December 2021 we have treated 51 nonsurgical GM patients, 34 men (67%) and 17 women (33%) with Hypofractionated and Intensified RT.
Median age was 60.1 (31-83 years old).
All of them received IMRT, in 20-25 fractions, (24.5 median fractions) in a dose escalated phase II trial, from a total dose of 66 Gy, to 79.65 Gy (median 69.8 Gy) EQD2 86 Gy), as follows:
PTV1 : 50 Gy in 2 Gy per fraction. PTV2 , as a concurrent boost receiving up to 79.65 Gy . 2.2 – 3.16 Gy per fraction.
40 patients received concurrent Temozolomide, 25 patients of them received at least three adjuvant Temozolomide cycles .
Organs at risk were delimited: Braim stem, chiasm and optical nerves, motor cortex, pyramidal path, pituitary, hippocampus and cerebrum.
After treatment, follow-up was done every 3 month with MRI .
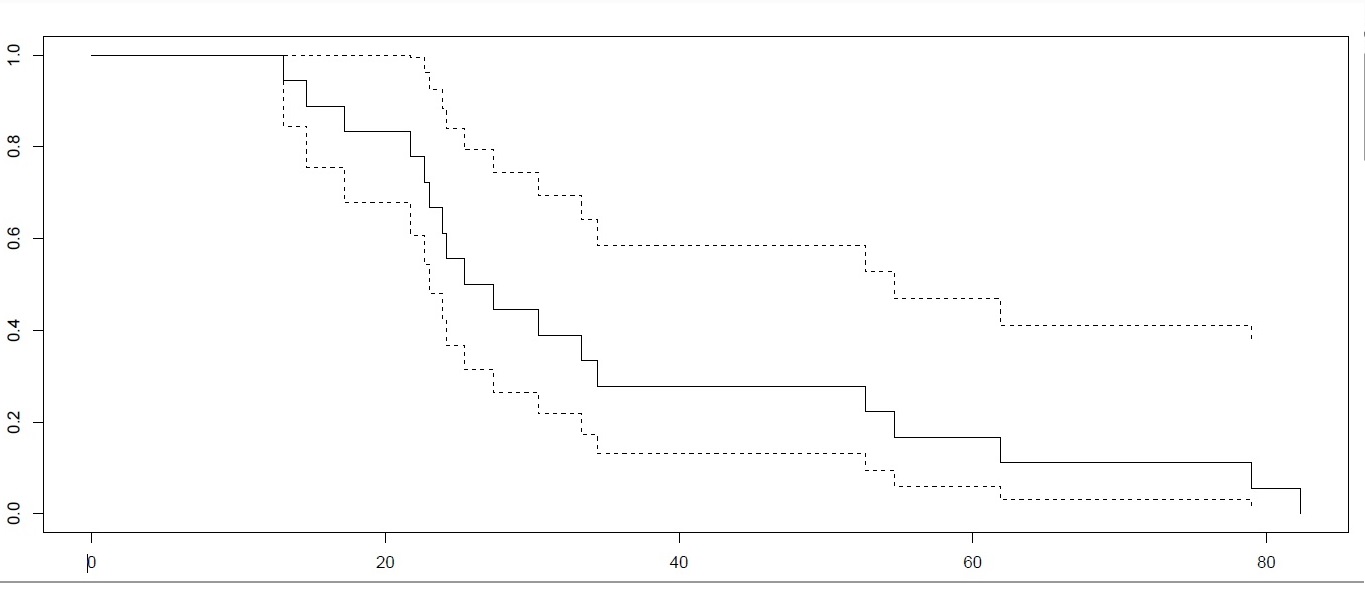
We have analyzed survival in two groups, depending on the fractionation: <2.5 and ≥2.5 Gy
Results
Hypofractionated and Intensified Radiotherapy was well tolerated. 90 % of the patients finished the treatment
All the breaks during radiation treatment were produced by the disease.
On follow-up MRIs, compatible changes due to treatment /radionecrosis, unable to rule out progression, were observed in 84% of biopsied patients.
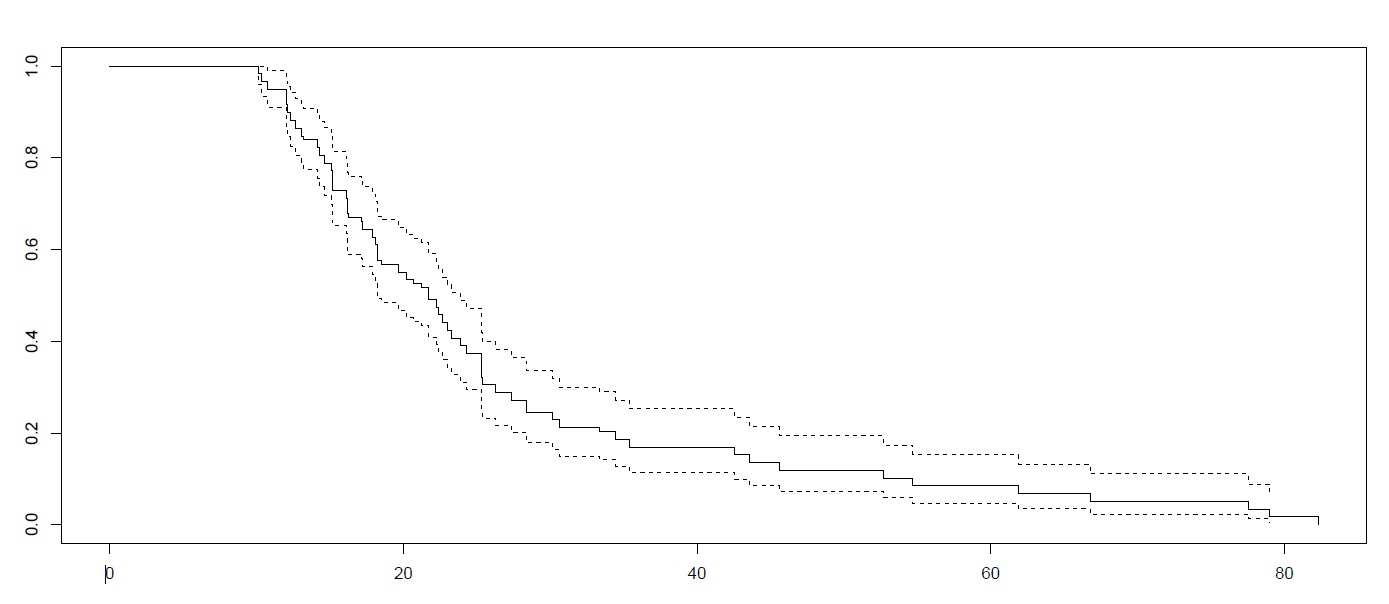
Overall Survival was 15.5 mounths (2-66 m).
21 patients with fractionation < 2.5 Gy OS was 13.1 months.
30 patientes with fractionation ≥ 2.5 gy, OS was 17.2 months
Conclusion
Hypofractionated and intensified radiotherapy improves OS in patients with nonsurgical GM, compared to conventional treatment (Stupp ).
This treatment doubles the overall survival in this group.
We recommend fractionation ≥ 2.5 Gy/day.