Dosimetric study of radiation dose to external auditory canal among nasopharyngeal cancer survivors
Sum Yin Serene Ho,
China, Hong Kong Special Administrative Region
PO-2346
Abstract
Dosimetric study of radiation dose to external auditory canal among nasopharyngeal cancer survivors
Authors: Sum Yin Serene Ho1,2, Wai Lam Yeung1, Chun Hay Mak1, Hiu Tung Ng1, Kairos Tsang1, Wan Shun Vincent Leung1, Catherine Po Ling Chan3, Shara Wee Yee Lee1
1The Hong Kong Polytechnic University, Department of Health Technology and Informatics, Hong Kong, China; 2Hong Kong Sanatorium & Hospital, Department of Radiotherapy, Hong Kong, China; 3The Chinese University of Hong Kong, Department of Otorhinolaryngology, Head and Neck Surgery, Hong Kong, China
Show Affiliations
Hide Affiliations
Purpose or Objective
External auditory canal (EAC) squamous cell carcinoma (SCC) is a rare tumour, accounting for less than 0.2% of all head and neck (H&N) cancers. Nasopharyngeal carcinoma (NPC) survivors who had previous radiotherapy (RT) have a 1000-fold risk of developing second primary EACSCC. This could be attributed to previous high dose irradiation to the H&N region. In this study, we first investigated the radiation doses to the EACs in those NPC survivors who eventually developed EACSCC. With the recent advancement of RT techniques, our second objective was to compare the doses to the EACs between conventional 2-dimensional RT (2DRT) and advanced intensity (IMRT)/ volumetric-modulated (VMRT) techniques in NPC RT.
Material and Methods
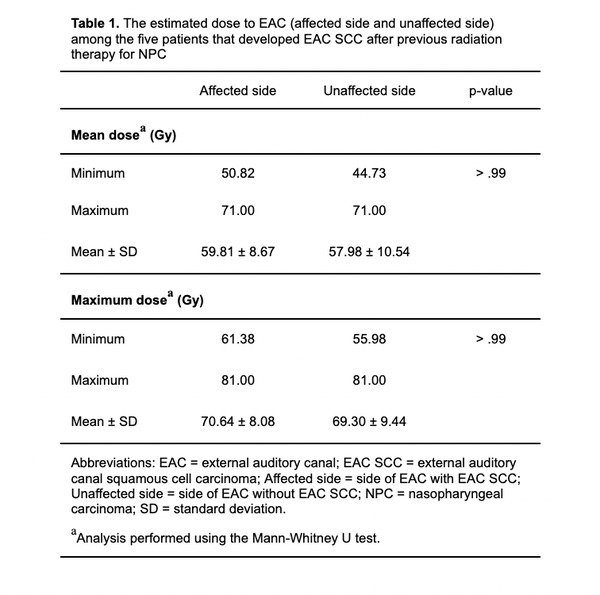
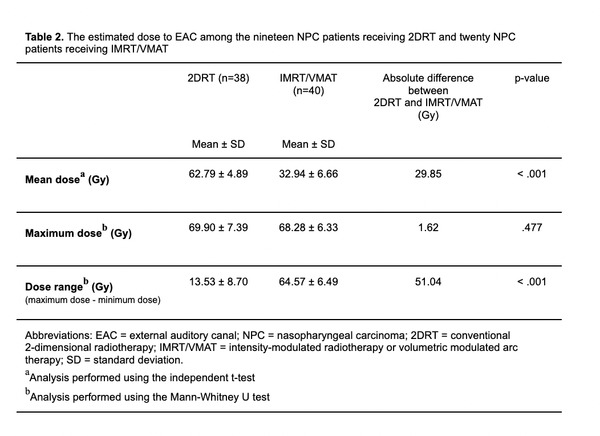
For part one, five cases with EACSCC who previously underwent 2DRT for NPC (prescribed dose >60 Gy) were retrospectively reviewed using planning images to estimate the radiation doses to the EACs. The mean and maximum dose to the EACs were compared between the affected and unaffected sides. In part two, twenty IMRT/VMAT and nineteen 2DRT plans treated between 1988-2020 were randomly extracted from a tertiary hospital for estimating the dose to the EACs. Similar to part one, the dose range (difference between the maximum and minimum dose points within the EAC), mean and maximum dose to the EACs between the two techniques were compared.
Results
For the NPC survivors with EACSCC treated with 2DRT, there were no statistical differences in the mean and maximum doses of EACs between the affected and unaffected sides (Table 1). Comparing between 2DRT and IMRT/VMAT techniques, the mean dose to the EACs using IMRT/VMAT (32.94Gy) was drastically lower than using 2DRT (62.79Gy), which would minimise acute ototoxicity. The dose range in the EAC region using IMRT/VMAT (64.57Gy) was significantly larger than 2DRT (13.53Gy) (p< .001), indicating that the EAC immersed in a relatively lower and more heterogeneous radiation bath, compared with 2DRT (Table 2). This may paradoxically increase the risk of developing second primary cancers from mutagenesis. Such a pattern has been observed in NPC survivors receiving IMRT, with an increase in thyroid cancer risk that was not present in 2DRT cases.
Conclusion
The NPC survivors with second primary EACSCC exposed to an equally high radiation dose to both EACs in previous 2DRT. With IMRT/VMAT, the mean dose to the EACs could be reduced by half, but the wider dose range implied an exposure of a low and heterogeneous dose to the EACs. Further study to evaluate the dominating factors that increase the risk of second cancer after IMRT/VMAT is warranted when sufficient follow-up is available.