Risk analysis of HDR prostate brachytherapy procedures
PO-2172
Abstract
Risk analysis of HDR prostate brachytherapy procedures
Authors: Tania Santos1, Carla Alves1, Cristina Miranda2, Maria do Carmo Lopes1
1Portuguese Institute of Oncology of Coimbra Francisco Gentil, E.P.E., Medical Physics Department, Coimbra, Portugal; 2Portuguese Institute of Oncology of Coimbra Francisco Gentil, E.P.E., Radiotherapy Department, Coimbra, Portugal
Show Affiliations
Hide Affiliations
Purpose or Objective
HDR prostate brachytherapy is performed at our institution for 16 years now, with about 20 patients treated per year. The purpose of this work was to perform a risk assessment of the HDR prostate brachytherapy procedures.
Material and Methods
The risk analysis methodology proposed in AAPM TG 100 was followed. First, a process map was built describing the main steps of the HDR brachytherapy procedure, from patient preparation, and treatment planning to dose delivery. Then, a failure mode and effect analysis (FMEA) was carried out to identify the potential failure modes (FM) in each step as well as the corresponding causes and eventual impact on the process outcome. This analysis was done assuming that no specific safety barriers were in place. For a given FM, the probability of occurrence (O), the likelihood of not being detected (D), and the severity (S) of the effect, were given a score from 1 to 10, based on TG 100. The risk probability number (RPN), used to rank the hazard of the identified FM, was calculated as the product of the O, D and S values. The top five highest-ranked FM were identified and corrective actions were suggested to reduce the associated risk.
Results
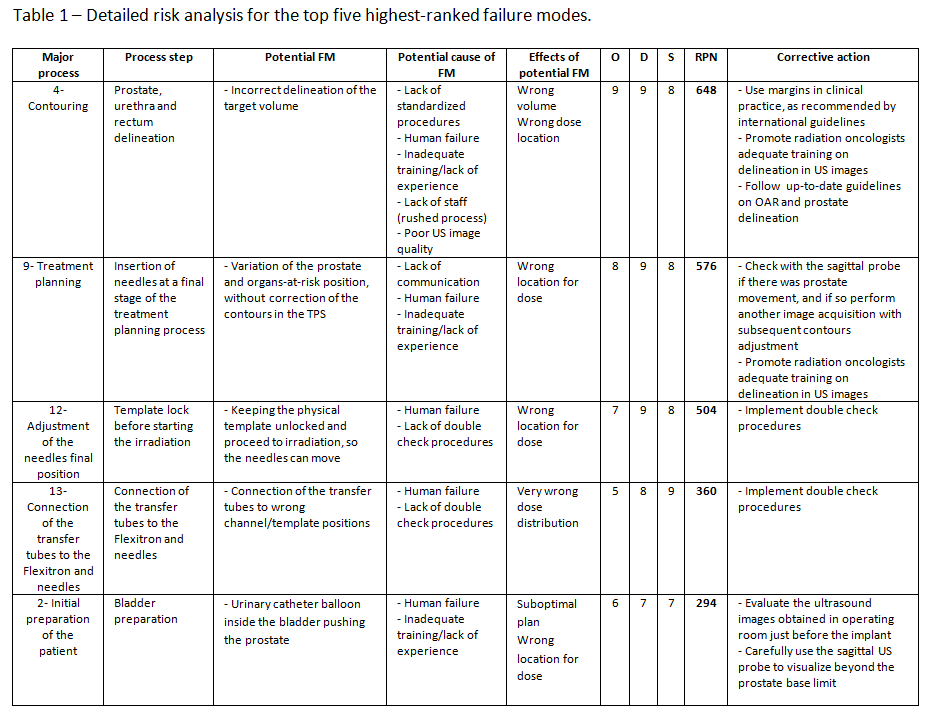
A total of 26 process steps and 35 FM were identified. From among the causes for the FM, human failure was the most frequent, followed by inadequate training, lack of staff and of standardized procedures, as well as inadequate communication between the team members. The potential effects of the FM varied from time delay with corresponding inconvenience for patient and staff (4/35) to very wrong dose distribution/absolute dose (8/35). The calculated RPN values ranged from 2 to 648. The five FM with the highest RPN were: 1- Incorrect delineation of the target volume (RPN 648); 2- Variation of the prostate and OAR position due to the insertion of needles at a final stage of the treatment planning, without correction of the contours in the TPS (RPN 576); 3- Keeping the physical template unlocked and proceed to irradiation, allowing eventual needles movement (RPN 504); 4- Connection of the transfer tubes to wrong channel/template positions (RPN 360); 5- Urinary catheter balloon inside the bladder pushing the prostate (RPN 294). From the five highest RPN failure modes, four had a severity score of 8 or 9. A summary of the results for these five FM is presented in Table 1. From the proposed corrective actions, some are already in place, but there are others like the use of margins that would need to be implemented. Overall, staff training, the establishment of double check procedures and promotion of a clear communication among team members were identified as key for mitigating the risk associated to various process steps.
Conclusion
The performed risk analysis has identified several ways in which the process could fail as well as corrective actions that should be implemented to improve the quality and safety of the HDR prostate brachytherapy procedures.