Dose gradients between HR-CTV 100% and IR-CTV 50% in IGBT of GYN cancer: Tandem vs Needles
PO-2129
Abstract
Dose gradients between HR-CTV 100% and IR-CTV 50% in IGBT of GYN cancer: Tandem vs Needles
Authors: Robert Kim1, Samuel Marcrom1, Mehran Yusuf1, Jeffrey Peacock1, Zohaib Iqbal1
1University of Alabama at Birmingham, Radiation Oncology, Birmingham, USA
Show Affiliations
Hide Affiliations
Purpose or Objective
Radiation therapy for locally advanced cervical cancer consists of concurrent chemoradiation therapy followed by brachytherapy (BT). Recently, 3D volume-based planning using image-guided brachytherapy (IGBT) has been increasingly used for adaptive treatment planning. For IGBT, GEC-ESTRO has proposed two different volume doses: the adaptive target volume dose at the time of brachytherapy, HR-CTV 85 Gy, and original volume before chemo-RT, IR-CTV 60 Gy. When EBRT was given 45 Gy before BT, 40 Gy from BT will make a total 85 Gy to the HR-CTV (EQD2). Therefore, 50% of the HR-CTV dose volume is a surrogate dose for the 60 Gy goal of the IR-CTV. The BT plans are primarily optimized for HR-CTV dose coverage, but the IR-CTV coverage depends on both the shrinkage of the original tumor in response to chemo-RT and dose fall off (dose gradient between 100% and 50%). This study investigates factors influencing the dose gradients for tandem and ovoid as well as needle plans.
Material and Methods
Three representative clinical cases were used for the gradient evaluation. The first case was a tandem and ovoid case planned using volume based optimization. From this tandem and ovoid case, five new plans were generated by placing reference points perpendicularly to the tandem source position at the same level as Point A and normalizing the dose to be 100% at each of these reference points. These reference points were placed at a distance of 0.5 cm, 1.0 cm, 1.5 cm, 2.0 cm, and 2.5 cm away from the source position. Next, the distances from the100% to the 50% isodose lines (IDLs) were measured. These measurements were performed along a perpendicular line from the source position. The second and third cases were interstitial cases with eight and seventeen implanted needles, respectively. The same process as described above was used to generate ten plans, however the reference points were placed perpendicularly with respect to the peripheral needle’s source position. Once again, the distances between the 100% to 50% isodose lines were measured.
Results
Table 1. The distance between the 100% isodose lines to the 50% isodose lines (gradient) are tabulated.
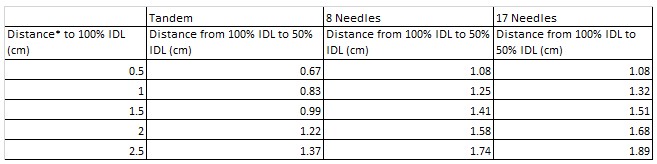
*Distance for Tandem is from source to 100% IDL and for Needles it is from the peripheral needle source to 100% IDL.
For both tandem and interstitial needle BT, the distance from the 100% to 50% isodose lines are larger when the distance from the tandem or most peripheral needle to the HR-CTV is larger. Additionally, with more needles, this distance is increased.
Conclusion
While more distance from the source to HR-CTV (prescription point) provides better coverage of the IR-CTV, it is
not recommended due to a larger internal hot spot, which may not be tolerated in some tissues.