Which carbon couch model can better quantify the influence on radiation dose?
Liubov Nesterenko,
Denmark
PO-1807
Abstract
Which carbon couch model can better quantify the influence on radiation dose?
Authors: Liubov Nesterenko1, Martin Berg1, Bjarke Mortensen1, Joachim Scholer Rasmussen1
1Hospital Lillebælt, Medical Physics, Vejle, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
Carbon couch tops are commonly used for patient support in external beam radiotherapy (RT). Accurate couch modeling in the treatment planning system (TPS) and validation of the dosimetric impact of the couch is important to deliver accurate RT. The purpose of this study is to find a model, which can quantify the carbon couch influence on radiation dose sufficiently.
Material and Methods
The iBEAM® evo couch top HP is a sandwich design couch, consisting of a Rohacell IG 71 foam core and surrounded by carbon fiber layers. Three models of couch layers were contoured in the TPS (RayStation, RaySearch Laboratories AB).
The mass densities (MD) were assigned based on Hounsfield Units (HU). Model 1 is a uniform model (MD of 0.152 g/cm3), model 2 consists of the outer carbon fiber layers (MD of 0.428 g/cm3) and inner foam core (MD of 0.089 g/cm3) while model 3 also assigns MD (0.732 g/cm3) to the lateral edges, where carbon fiber layers match each other and the ratio of carbon fiber to epoxy is higher due to monolithic compression in this area [Fig. 1]. Finally, model 4 is based on HU only.
The attenuation (ATT) of photon beams (6MV, 10MV, and 10MV FFF energies) by the couch top was measured and compared to the calculated data in the TPS for all four models. Three pelvic plans with different models of the couch were recalculated, and changes in PTV coverage and OAR dose were analyzed.
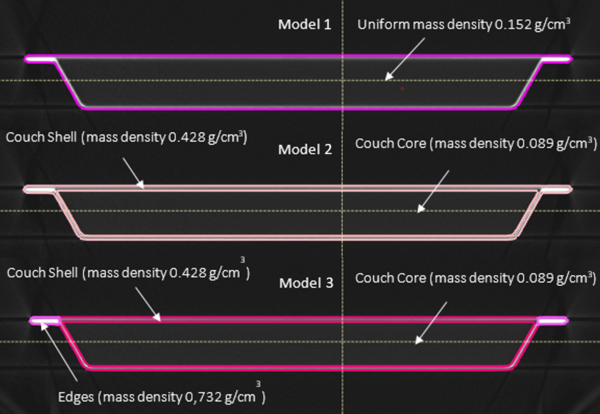
[Fig. 1]
Results
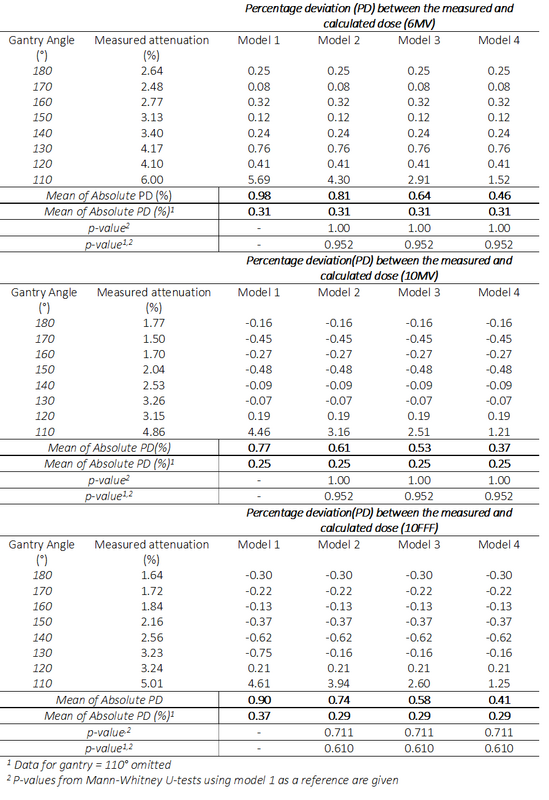
The agreement between measured ATT and TPS computed ATT was within 1% for all gantry angles for all models of the couch except at gantry angle 110°, where the field passes through the edges of the couch. Although more complex couch models showed increasingly better agreement between the measured and the TPS-calculated ATT, model 4 showed the lowest mean absolute percentage deviation (MAPD) for all energies [Table 1].
Parts of the couch are usually excluded from the CT field of view; therefore, accurate calculations cannot be possible without modeling the couch in TPS.
Three pelvic plans (2 full arcs, 4 partial arcs, 3DCRT) with model 1-3 were compared. No significant changes in PTV coverage or OAR dose were observed in the full arcs VMAT plans. The result of the analysis of the VMAT plan with 4 arcs passing through the edges of the couch shows a slight difference in PTV coverage, while the 3DCRT plan with two fields crossing the edges of the couch shows the largest difference in PTV coverage. No significant changes in OAR dose were observed.
Conclusion
We suggest to use the couch model 1 in clinical practice although it demonstrates a higher MAPD of 0.98% for 6 MV compared to both model 3 and model 2 (MAPD 0.64% and 0.81% respectively) as a multi-density couch model enhances the risk of not placing high-density parts of the couch top consistently throughout the complete treatment course. Fields for 3DCRT passing solemnly through the edges of the couch should be avoided.
For high-accuracy treatments such as SBRT where higher accuracy is needed couch model 3 might play a role.
Table 1