CTV-free lung planning: Can we reduce toxicity whilst maintaining local control?
Matthew Craddock,
United Kingdom
PO-2117
Abstract
CTV-free lung planning: Can we reduce toxicity whilst maintaining local control?
Authors: Matthew Craddock1,2, Corinne Faivre-Finn1,2, Marcel van Herk1,2, Alan McWilliam1,2, Gareth Price1,2
1University of Manchester, Division of Cancer Sciences, Manchester, United Kingdom; 2Christie Hospital NHS Trust, Department of Clinical Oncology, Manchester, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
CTV-free planning in lung cancer has been proposed as a method of reducing toxicity whilst maintaining treatment effectiveness. The rationale for CTV-free treatment derives from the lower cell density and differences in radiobiological response of microscopic disease (MD), which give the same level of cell killing at lower doses than in bulk tumour. This contradicts the conventional ICRU62 recipe for target volumes but early clinical studies report no loss in local or marginal control and significantly lower rates of acute radiation pneumonitis. However, the mechanism driving these positive results has yet to be explained and the impact on plan robustness and potential benefit of patient stratification remains unclear.
This study aims to evaluate the feasibility of CTV omission in locally advanced SIII NSCLC (T3N0M0) patients using a simulation approach which accounts for errors in treatment preparation and delivery. TCP modelling is used to estimate the potential clinical impact, with the distribution of microscopic disease directly included in the analysis for the first time.
Material and Methods
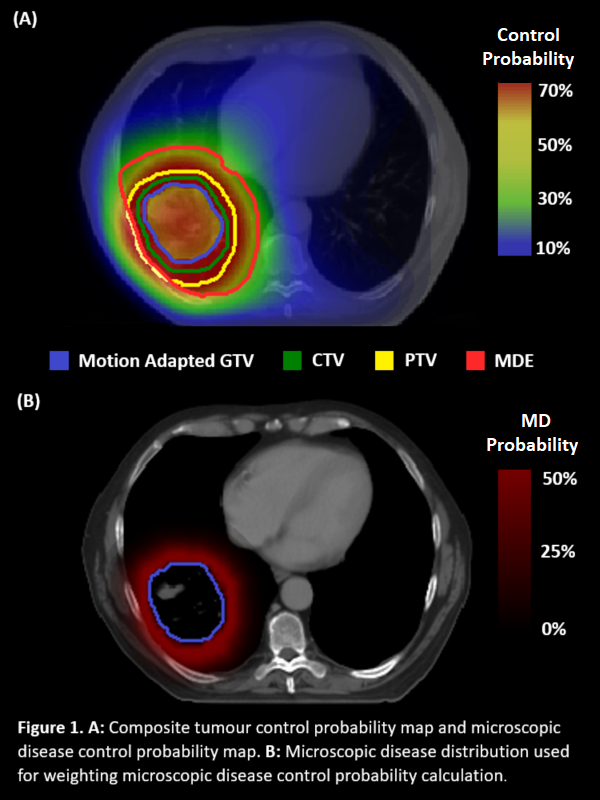
10 pairs of conventional and CTV-free VMAT treatment plans were prepared with a prescription dose of 55 Gy in 20#. The CTV consisted of a 5 mm expansion of the motion adapted GTV (MAGTV) (this was omitted in the CTV-free plans) with a further 5 mm expansion to form the PTV. Random uncertainties were modelled by blurring the dose distribution with a gaussian filter of width 3 mm and systematic uncertainties were simulated by randomly selecting 100 shifts in all 3 cardinal directions from a normal distribution with a SD of 3 mm. Voxel-wise TCP values were calculated separately for bulk tumour and MD with a Poisson TCP model using parameters from Okunieff et al (1995). To encompass the maximum extent of MD in >95% of patients a MD region was defined as a 3 cm rind around the MAGTV, limited to the boundaries of the lungs. The calculation of MD control probability (MCP) was weighted by the probability of MD presence, with geometric averages used to summarise the control probability distributions for each shift and the arithmetic average over all shifts taken to summarise results at the patient level.
Results
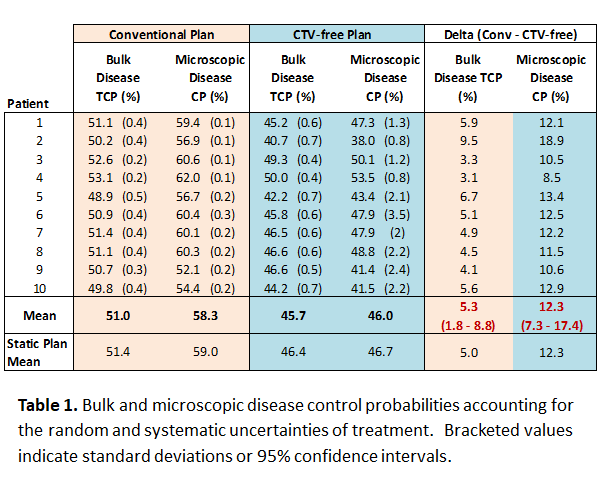
The average reduction in CTV-free TCP and MCP from conventional planning was 5% (95% CI: 1.8–8.8%) and 12% (95% CI: 7.3–17.4%), accounting for random and systematic uncertainties of treatment. Average dose reductions were 2.1 Gy (range: 1.2-4.1 Gy) in mean dose to healthy lung, 4% (2–10%) in V20; 2.3 Gy (0.4–3.9 Gy) in mean heart dose and 2.7 Gy (0.9–4.3 Gy) in mean oesophagus dose.
Conclusion
The results suggest the omission of the CTV produces only a moderate decrease in the control probability of macro- and microscopic disease. Although further validation of this methodology in larger patient cohorts is required, our findings are concordant with the results of clinical studies. Further study to better understand the risks and benefits of CTV-free treatment planning is warranted.