Hypofractionated dose-intensified palliative RT: 25 Gy in 5 fractions for enhanced symptom control
Jayson Paragas,
Philippines
PO-1602
Abstract
Hypofractionated dose-intensified palliative RT: 25 Gy in 5 fractions for enhanced symptom control
Authors: Jayyson Paragas1, Vanessa Di Lalla1, Marc David1, Sonia Skamene1, Leticia Alvarado1
1McGill University Health Centre, Division of Radiation Oncology, Montreal, Canada
Show Affiliations
Hide Affiliations
Purpose or Objective
Selection between standard palliative dose schedules versus more aggressive palliative approaches is an ongoing dilemma, with recent shift towards the latter to provide improved symptom relief and local control, especially among patients with longer life expectancy. Stereotactic approaches show promise in these respects, however, these techniques are highly resource-intensive and may not be widely available. We assessed the tolerance and efficacy of non-stereotactically planned 25 Gy in 5 fractions to strike a balance between higher biologically effective dose (BED) with acceptable side effect profile and shorter treatment duration.
Material and Methods
Our local radiotherapy database was retrospectively reviewed over a 10-year period (September 2011 to August 2021) for patients receiving 25 Gy in 5 fractions treated with palliative intent. Patients who received stereotactic ablative treatment techniques, curative-intent therapy, and patients who were asymptomatic at the treated sites were excluded.
Results
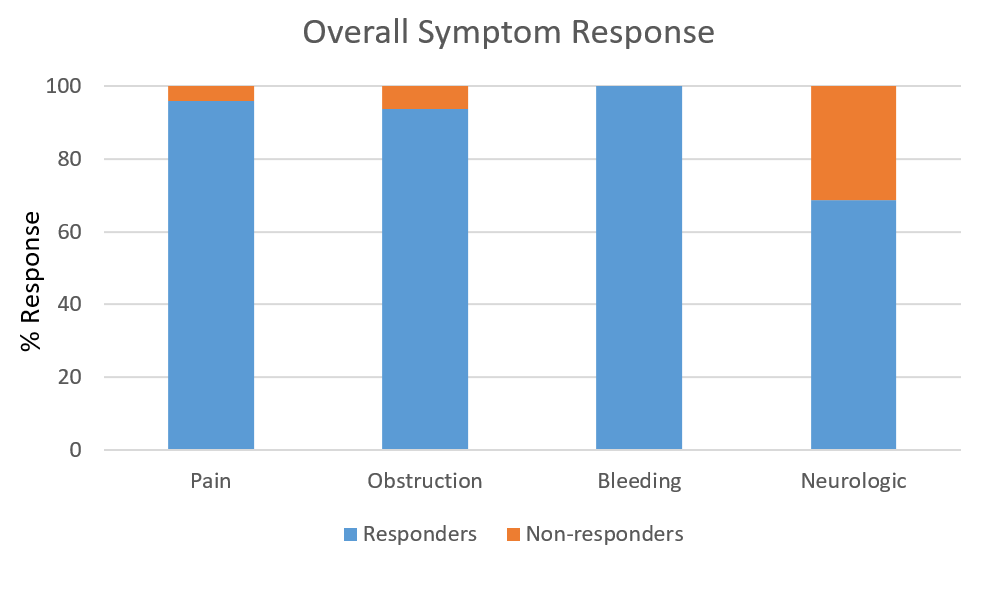
A total of 127 patients corresponding to 136 treated sites were included in this analysis. A third of the patients were >80 years old (median 70 years, range 35 – 98 years), 51% ECOG ≥ 2, 66% Charlson comorbidity index ≥8 and 77% metastatic at time of treatment. Most commonly treated sites were rectum (20%), non-spine bone (18%), spine (12%), lymph node (12%) and esophagus (8%), and 88% had no previous RT at the same site. Median GTV 110.1cc (range 4 – 2940.8cc) and median PTV 321.8cc (range 14.7 – 3991cc). Treatment was delivered using VMAT (74.5%), IMRT (10.9%) 3DCRT (10.2%), or 2D (4.4%). At a median follow-up of 20 weeks (1 – 308 weeks), the overall response rate was 96% for pain control, 93% for obstruction relief, 100% for bleeding control and 69% for improvement of neurologic deficits. Toxicities ≥ Grade 3 occurred in 3.6% of the cohort (odynophagia, dyspnea, progression of intestinal obstruction and wound infection progression). Median OS was 9 months. Fifty (37%) patients survived more than 1 year. Only 1 patient died within 30 days from cause unrelated to palliative radiotherapy meeting the quality indicator for radiation futility. On multivariate analysis, only ECOG score was significantly associated with treatment response (OR 0.40, p=0.036).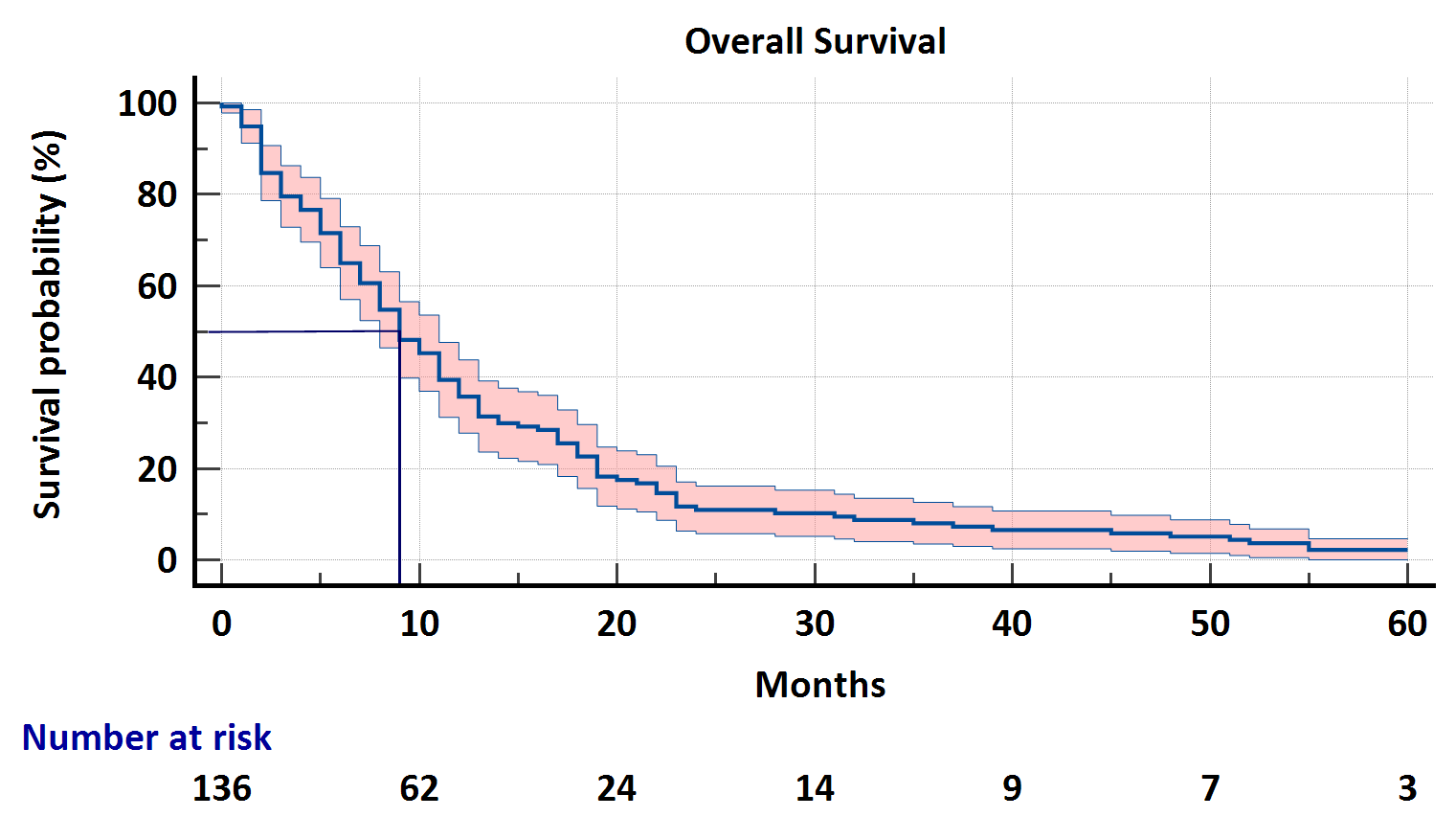
Conclusion
To our knowledge, this is the largest study reporting on the use of non-stereotactically delivered 25 Gy in 5 fractions palliative radiotherapy. Our data suggests that this dose fractionation is tolerable and effective for symptom control, even among elderly frail symptomatic patients when compared to historical data using alternative palliative dose fractionation schemes. Further exploration of non-stereotactic moderate hypofractionation for palliation is needed to optimize palliation in patients without access to or those ineligible for stereotactic approaches.