Optimizing palliative radiotherapy treatment in last 30 days of life
Jose David González,
Spain
PO-1594
Abstract
Optimizing palliative radiotherapy treatment in last 30 days of life
Authors: Jose David González1
1Hospital Universitario Arnau de Vilanova, Radiation Oncology, Lleida, Spain
Show Affiliations
Hide Affiliations
Purpose or Objective
30-days mortality rate (30DMR) is known as an overtreatment endpoint for palliative patients. The recommended 30DMR is under 20%. In a previous analysis done in our center we found our 30DMR is 18.88%. We aimed to study if 30 and 15DMR could be related to primary tumor site and if this could be a factor in the decision making about what patients to offer a palliative radiotherapy treatment
Material and Methods
We recorded the survival length in days from the end of palliative RT of patients treated from January to December 2021 at our institution. We also collected the primary tumor site of every treatment done. Data was obtained from ARIA electronic data base.
Results
181 palliative treatments were performed, 143 patients were evaluable. Median age was 69 years-old. 57% were men and 43% women. Main treatment locations were: bone (30.77%), CNS (14.69%), lung (9%), colorectal (6.3%) and bladder (2.1%). The most common primary tumors treated were: lung (30.77%) colorectal (14.69%) breast (13.99%) prostate (9%) and gastroesophageal (6,3%) the rest of tumors encompassed the 23.08%. If we look at the cohort of patients that died in the first 30 days (18.88%) the primary tumor distribution was: Lung (44.44%) Rectal (14.81%) Breast (14.81%) Gastric (11.11%) Others (14.81%). In the analysis between primary sites the 15 and 30DMR were as follows: Lung (18.1% and 24.9%) Colorectal (0 and 26.6%), breast (10 and 20%), Prostate (0 and 0%) gastroesophageal (0 and 33.33%).
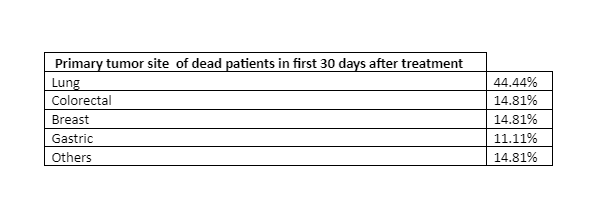
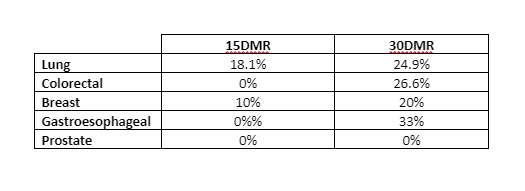
Conclusion
Lung is the most prevalent tumor between the patients that died in the first 30 days after treatment. Lung cancer was the tumor with the highest 15DMR. Lung, colorectal and gastroesophageal tumors had a 30DMR higher than the recomended 20%. This could indicate that it could be a factor in the decision whether to treat these patients. On the other side prostate cancer had a 0% 15 and 30 DMR so it seems correct to offer palliative radiotherapy to this group. Further investigation is needed in order to find other prognostic factors that help us decide which patients we should offer palliative radiotherapy.