Applicability of SBRT for early prostate cancer and correlation with CTV variation during treatment
PO-1533
Abstract
Applicability of SBRT for early prostate cancer and correlation with CTV variation during treatment
Authors: Antonio Angrisani1, Roberto Miceli2, Laura Cedrone2, Carla Rinaldi2, Antonia Frisone2, Olga Ruggieri2, Rolando Maria D'Angelillo3
1"L. Vanvitelli" University of Campania, Precision Medicine - Radiotherapy Unit, Naples, Italy; 2Fondazione Policlinico “Tor Vergata”, Radiotherapy, Rome, Italy; 3Fondazione Policlinico “Tor Vergata”, Department of Radiotherapy, Roma, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Stereotactic body radiation therapy (SBRT) for the treatment of early-stage prostate cancer (PCa) has increased over the last 5 years. The need to shorten the patient's stay in the clinic, the cost/effective benefits, the updates from non-inferiority trials on SBRT versus the conventional RT and the high compliance of patients encourage its use. However, the largest series of PCa patients treated with SBRT come from specialized centers often using uncommon technology (e.g. MRI-Linacs). We aim to investigate the applicability of Linac-based SBRT for PCa using the standard level of technology and image guide (namely CBCT), with a focus on the evolution of the CTV variation over the treatment time.
Material and Methods
Patients with early-stage PCa at low/intermediate risk treated with linac-based ultra-hypofractionation and daily set-up control through CBCT were prospectively evaluated. The main exclusion criteria were nodal or distant metastasis, history of prostate surgery (except TURP), other malignancies less than 5 years before RT, a prostate volume >80cc, uroflowmetry Qmax <10ml/sec, and previous pelvic irradiation. The plans were calculated either with the 7-and 5-fractions schedule. RT was delivered for a total dose of 42.7 Gy in 7 fractions every other day, with VMAT technique (6-10 MV energy, flattening filters free). The specific dose constraints used were extracted from the protocols of the two main trials (HYPO-RT, PACE-B), involving the plan optimization to spare the intraprostatic urethra PRV, as well as the other overlapping regions PTV/OARs (rectum, bladder). The CBCT scans obtained were also used to see if any CTV changes occurred, delineating the CTV structure for each fraction. The volume variables obtained were analyzed with the Friedman test and Wilcoxon test. The biochemical response and the clinical evaluation of early toxicity (CTCAE v.5) and patient-reported outcomes, were collected 60 days after the end of RT.
Results
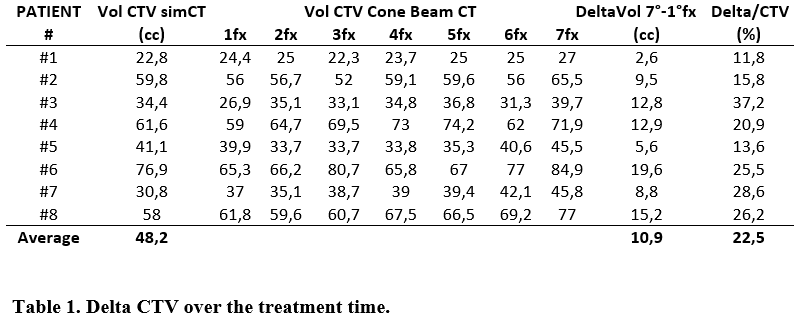
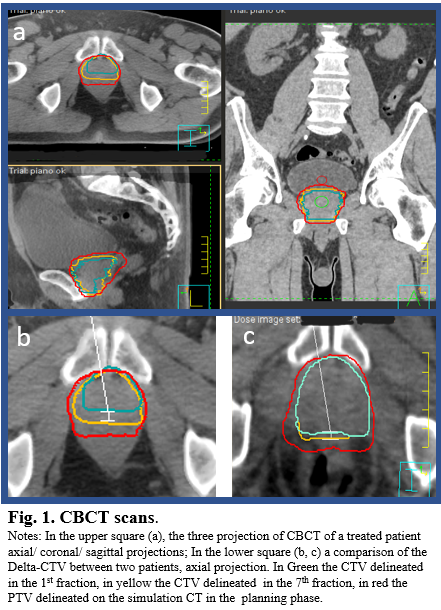
Eight patients were included in the present analysis, and 56 CBCT were collected. The CTV analysis showed a significant increase of the volume from start to end of 22% on average (p=0.012) and during the treatment (p<0.01) supposedly for an RT-induced inflammation, most frequently among the 5th and 6th fraction (table 1), mostly localized at the posterior-apical edge of the gland abutting the rectum. Despite the CTV changes, the clinical target was always encompassed within the PTV (Fig.1). No toxicity G1>1 was recorded. The PSA post-RT decreased 7 folds in 2 months from RT on average.
Conclusion
SBRT for PCa is feasible, and it can be applied in all the RT facilities with standard-level equipment, translating the innovative technique into a frequent action. The specific dose constraints require special caution. A significant increase in CTV volume during treatment time can occur, with no impact on target coverage. We encourage larger real-world data to improve the use of SBRT for PCa.