Ultra Hypo RT in elderly PCa patients with aggressive disease: still a space for curative approach?
PO-1492
Abstract
Ultra Hypo RT in elderly PCa patients with aggressive disease: still a space for curative approach?
Authors: Giulia Corrao1, Giulia Marvaso1, Chiara Lorubbio1,2, Federico Mastroleo1, Maria Giulia Vincini1, Cristiana Fodor1, Ilaria Repetti1,2, Vanessa Pierini1, Giovanni Carlo Mazzola1, Cristiana Pedone1, Dario Zerini1, Barbara Alicja Jereczek-Fossa1,2
1IEO, European Institute of Oncology, IRCCS, Division of Radiation Oncology , Milan, Italy; 2University of Milan, Department of Oncology and Hemato-oncology, Milan, Italy
Show Affiliations
Hide Affiliations
Purpose or Objective
Longer life expectancy has led to a significant increase in the number of elderly patients localized PCa candidates for curative RT. Patients aged ≥ 75 years often present a high prevalence of comorbidities and it makes difficult to propose RT including both prostate and pelvis associated with long-term androgen deprivation therapy (ADT), as recommended by NCCN guidelines.
The aim of the present study (Ethical Committee approval number UID 2684) is to evaluate the efficacy and safety of personalized ultra hypofractionated RT (UHRT) +/- ADT in this cohort of patients.
Material and Methods
Elderly men aged ≥75 years with unfavorable intermediate to high-risk localized PCa who underwent UHRT on prostate between 2012 and 2018 were identified and analyzed. Continuous variables were summarized as mean/median and interquartile range/range, while categorical variables were presented with absolute and relative frequencies. Toxicities were collected according to RTOG scale and survival curve was calculated with Kaplan-Meier method for biochemical recurrence.
Results
A total of 108 patients fullfilled inclusion criteria. Among them, 56 (52%) were diagnosed with unfavorable intermediate and 52 (48%) with high-risk PCa. Median age at diagnosis was 80 years (Range 75 - 90) and median PSA at diagnosis was 9.2 ng/ml (Range 1.2-220.4).
All patients underwent UHRT on prostate in 5 fx every other day with a dose/fx within 6.5 and 7.25 Gy. The majority of patients (61%) underwent concomitant ADT with a median duration time of 9.0 months (1.0-4.6). General cohort characteristics and reported toxicities are summarized in Table 1.
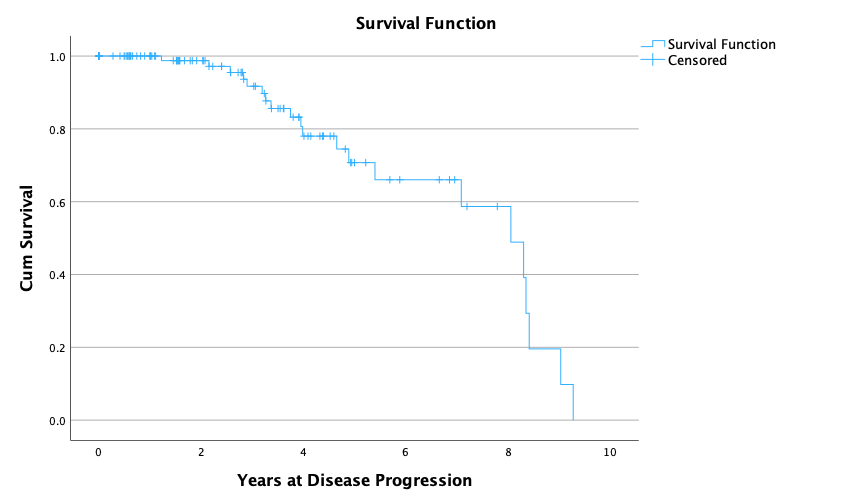
After a median follow-up of 2.8 years (IQR 1.0-4.3), 21 patients (19.4%) experienced a biochemical recurrence, with a median time to biochemical recurrence of 29.8 months (IQR 20.4 – 42.9). One and 2 years biochemical DFS rates were 99.99% and 99.95%, respectively. Kaplan-Meier survival curve can be seen in . Among the 21 biochemical recurrences, 13 patients (12.0%) developed a clinical progression of disease (10 in high risk and 3 in unfavorable intermediate risk classes). At last censored FU, 65 patients (60.0%) are alive with no evidence of disease, 15 (13.9%) are alive with disease and 18 (16.6%) died.
One G2 gastrointestinal (GI) acute toxicity was observed and 6 G2 genitourinary (GU) toxicities were reported. No G≥3 GU/GI acute toxicities were noted. A G2 late toxicity occurred in 2 patients for both GI and GU toxicities. One G3 GU late toxicity was described. All toxicities were solved at last follow-up.
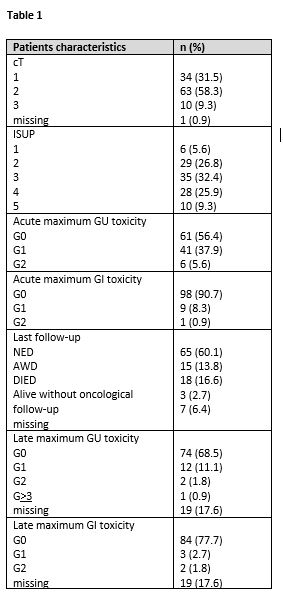
Figure 1
Conclusion
Elderly patients show optimal biochemical control and safe GI/GU toxicity profiles. In conclusion, in this setting of patients, with the aim to propose a curative treatment and, at the same time, to preserve the quality of life in these frail patients, personalized ultra UHRT +/- short ADT course should be considered as a treatment option, according to oncological characteristics and comorbidities.