Prediction of daily GI doses in SBRT for pancreatic cancers using the shortest distance to GTV.
PO-1389
Abstract
Prediction of daily GI doses in SBRT for pancreatic cancers using the shortest distance to GTV.
Authors: Yusuke Uchinami1, Takahiro Kanehira2, Keiji Nakazato2, Yoshihiro Fujita1, Shuhei Takahashi1, Hiroshi Taguchi3, Keiji Kobashi4, Norio Katoh1, Keita Takahashi5, Hidefumi Aoyama6, Naoki Miyamoto2, Kohei Yokokawa2
1Hokkaido University Faculty of Medicine and Graduate School of Medicine, Department of Radiation Oncology, Sapporo, Japan; 2Hokkaido University Hospital, Department of Medical Physics, Sapporo, Japan; 3Hokkaido University Hospital, Department of Radiation Oncology, Sapporo, Japan; 4Hokkaido University Faculty of Medicine and Graduate School of Medicine, Global Center for Biomedical Science and Engineering, Sapporo, Japan; 5Hokkaido University Graduate School of Medicine, Department of Biostatistics, Sapporo, Japan; 6Hokkaido University Faculty of Medicine and Graduate School of Medicine, Department of Radiation Oncology,, Sapporo, Japan
Show Affiliations
Hide Affiliations
Purpose or Objective
Stereotactic body radiotherapy (SBRT) for pancreatic cancers is expected to improve treatment outcomes, but dose uncertainty due to inter-fractional motion should be considered. This study aims to verify whether the daily gastrointestinal tract (GI-tract) doses can be predicted based on the shortest distance between gross tumor volume (GTV) and GI-tract.
Material and Methods
The analyzed cases included ten pancreatic cancer patients receiving a fiducial-based respiratory-gated SBRT of 40 Gy in 5 fractions. The planning CT was scanned at the natural expiration, and the SBRT plan was generated by step-and-shoot intensity-modulated radiotherapy (IMRT) with 9-10 portals. Here, we defined this reference treatment plan as PLANref. Before every fraction, CT images for dose evaluation were obtained at the same position and respiratory phase as in the planning CT. Using PLANref, the dose was evaluated by re-calculating PLANref on the daily CT with the same positional relationship between the isocenter and the fiducial marker. We also defined the re-calculated evaluation plan as PLANeval. The three-dimensional shortest distance was calculated from GTV to each GI-tract (gastro-duodenum, small intestine, and large intestine) using a commercially available MIM maestro ver. 7.0 (MIM Software, Cleveland, OH, USA). The institutional dose constraint is volume receiving 33 Gy (V33) < 0.5 cm3 for the planning at risk volume (PRV) of each organ, which was generated by adding a 5 mm margin. Therefore, the PRV dose received by 0.5 cc (D0.5cc, the maximum dose delivered to 0.5 cc) was also evaluated. For quantitative evaluation between PLANref and PLANeval, the difference of the shortest distance (delta shortest distance) and D0.5cc (delta D0.5cc) was calculated. Spearman correlation test was used to analyze the association between delta shortest distance and delta D0.5cc. The paired differences were analyzed with paired Wilcoxon signed-rank tests.
Results
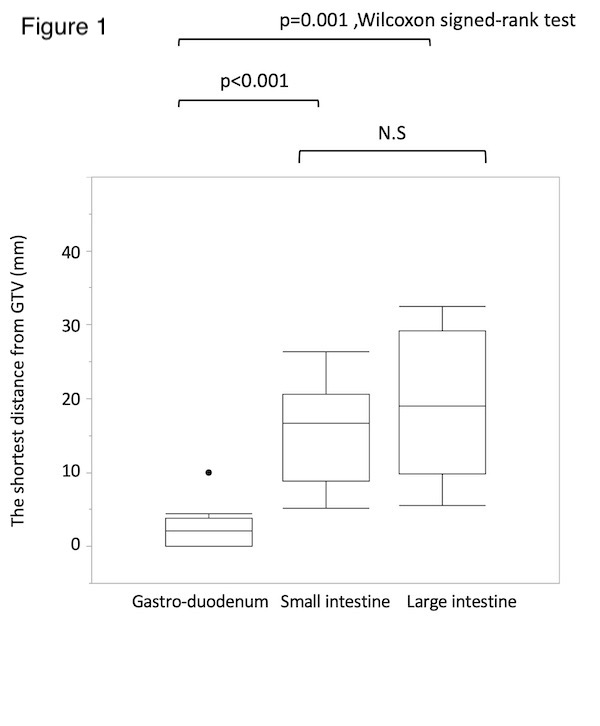
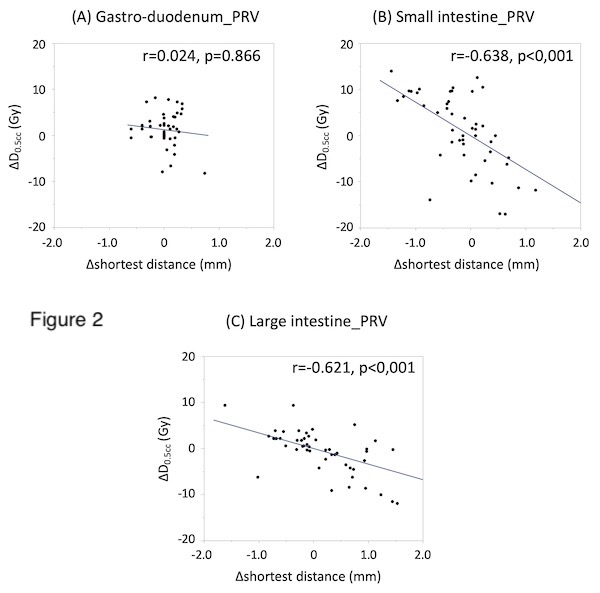
The median shortest distance in PLANref was 2.1 mm (interquartile range: IQR:0-3.8) in the gastro-duodenum, 16.5 mm (8.8-20.6) in the small intestine, and 19.0 mm (9.8-29.2) in the large intestine (Figure 1). The median D0.5cc of PRV in PLANref was 32.0 Gy (IQR: 31.7-32.4) in the gastro-duodenum, 25.6 Gy (18.9-29.9) in the small intestine, and 19.7 Gy (16.3-28.5) in the large intestine. In spearman correlation test, significant association between delta shortest distance and delta D0.5cc was found in the small (correlation coefficients r=-0.638, p<0.001) and large intestine (r=-0.621, p<0.001), but not in the gastro-duodenum (r=0.024, p=0.866) (Figure 2)
Conclusion
The gastro-duodenum is more likely to receive high-dose, possibly due to its proximity to the GTV. Prediction of daily gastro-duodenum dose was suggested to be difficult solely from the shortest distance in daily CT images.