Early experience of setting up a Cardiac SABR service and treatment of Ventricular Tachycardia
Marina Khan,
United Kingdom
PO-1082
Abstract
Early experience of setting up a Cardiac SABR service and treatment of Ventricular Tachycardia
Authors: Marina Khan1, John Whitaker2, Aldo Rinaldi2, Mark O'Neil2, Shahreen Ahmad1
1Guys and St Thomas' NHS Foundation Trust, Radiotherapy & Oncology, London, United Kingdom; 2Guys and St Thomas' NHS Foundation Trust, Cardiology, London, United Kingdom
Show Affiliations
Hide Affiliations
Purpose or Objective
Cardiac SABR (cSABR) is a new treatment for intractable ventricular tachycardia (VT). Myocardial fibrosis or scarring caused by ischaemic damage gives rise to electrical re-entry and subsequent arrhythmia. Indication for radiotherapy for this benign condition is after conventional treatments have been exhausted. Reported data show up to 90% success rate in termination of VT. The precise mechanism of action is unclear and further pathophysiological studies are underway.
Material and Methods
4 centres in UK are currently offering this treatment. We discuss our experience of setting up the service at our centre and early results.
The treatment is available on a compassionate basis and is not a commissioned NHS service. We obtained departmental governance (Cardiology & Oncology) and senior hospital level approval. We developed a partnership with Cardiology colleagues at our Institution to identify suitable patients. Patients are discussed at a virtual UK cSABR MDM that takes place monthly to review each case.
We devised a clinical protocol to include clinical indications and patient selection. The protocol specified the planning process and treatment in detail.
The finalised process included advice from other centres offering this service and from our personal experiences as a well-established SABR site.
Patients are immobilised as per standard upper body. A 4DCT scan is acquired with abdominal compression when needed, and IV & oral contrast given. Volumes are contoured on the average dataset derived from all respiratory phases of the 4DCT planning scan. GTV, ITV and PTV are outlined jointly by oncologist and cardiologist as well as OARs including ICD and pacing leads. Using a combination of cardiac CT, 12-lead ECG and electrophysiological mapping data a target for treatment in the ventricle is identified.
Patients are planned with a VMAT technique using FFF photons; particular attention is needed to maintain oesophagus and stomach doses remain within tolerance. RPM was used to gate the treatment and AlignRT was used to track the patient’s position.
Results
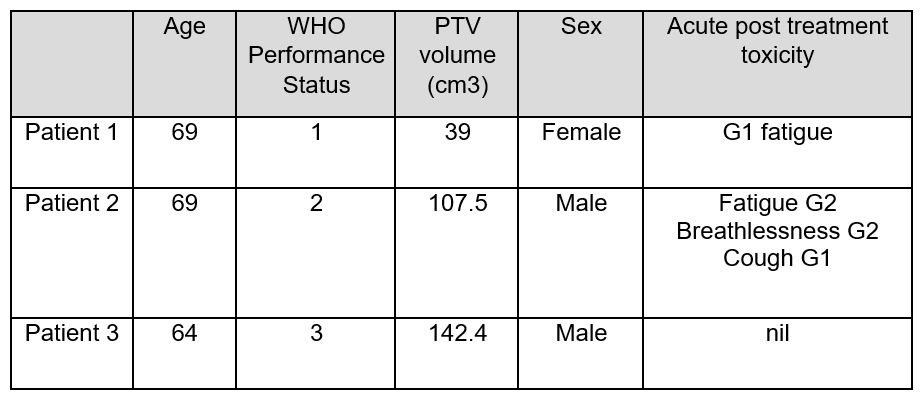
A dose of 25Gy in a single fraction is delivered to the PTV. 3 patients have been treated to date. All patients were successfully treated to the prescribed dose. All treated patients remain alive at a minimum of 6 months post treatment. 1 patient has remained free from sustained VT events since treatment 8 months ago. 2 patients have had some VT events since treatment and we continue to analyse their response.
Conclusion
cSABR is an innovative treatment for intractable VT. It is well tolerated and non-invasive unlike some other established treatments for this condition. Our experience shows modest success in the short term. The late effects of high doses of radiation to the heart remain unknown and in future treated patients will need close follow up in a clinical trials setting. As more patients are treated with cSABR we hope to find its place in the ongoing management of this debilitating and life-threatening condition.