Automatic VMAT treatment planning for left-sided breast cancer with lymph nodal involvement.
PO-1881
Abstract
Automatic VMAT treatment planning for left-sided breast cancer with lymph nodal involvement.
Authors: Kenni Engstrøm1, Carsten Brink1,2, Mette Holck Nielsen3, Martin Kjellgren1, Karina Lindberg Gottlieb4, Irene Hazell5, Vibeke Nordmark Hansen1, Ebbe Laugaard Lorenzen4
1Laboratory of Radiation Physics, Department of Oncology, Odense University Hospital, Odense, Denmark; 2Department of Clinical Research, University of Southern Denmark, Odense, Denmark; 3Department of Oncology, Odense University Hospital, Odense, Denmark; 4Laboratory of Radiation Physics , Department of Oncology, Odense University Hospital, Odense, Denmark; 5Laboratory of Radiation Physics, Department of Oncology, Odense University Hospital, Denmark, Odense, Denmark
Show Affiliations
Hide Affiliations
Purpose or Objective
Conventional
radiotherapy for breast cancer is tangential forward planed fields with segments.
This is often a manual and time-consuming process, which may be more consistent
with automatic planning. Treatment techniques such as Volumetric Modulated Arc
Therapy (VMAT) can be used to increase the coverage and conformity, but may increase
the dose to contralateral organs. In the present study, we evaluated VMAT in a
butterfly field configuration using Pinnacle Autoplan module in comparison with
forward planned tangential plans (3DCRT) in terms of dose to organs at risk,
target coverage, the number of breath holds required for treatment in deep
inspiration breath hold and dosimetric accuracy.
Material and Methods
Twenty
left-sided breast cancer patients, ten with mastectomy and ten with lumpectomy,
were used for the study. Seventeen of the patients were treated in deep
inspiration breath-hold. Patients were prescribed 50 Gy to the CTV’s. For all
patients, a VMAT and a forward tangential plan were generated. The forward plan
used step-and-shoot 6 MV combined with 18 MV fields for larger breasts. The
VMAT plan was made using two 6 MV VMAT fields in a butterfly configuration
(each arc spanning 40-70 degrees). A skin flash of 1cm was used to ensure
robustness for the VMAT plans. Dose planning was done in Pinnacle 16.0 using
the Auto-Planning module. Comparison of 3DCRT and VMAT was made by evaluating
the difference in dose to OAR and targets in terms of mean dose, metrics
provided by DBCG guidelines1, dose-volume histograms, and required breath-holds
for treatment delivery.
Results
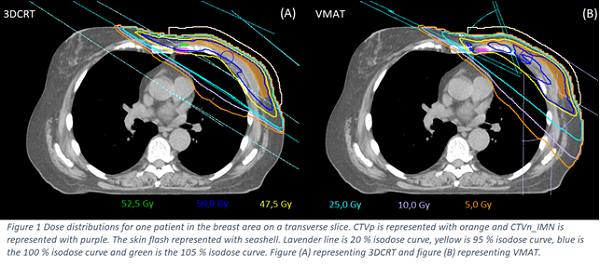
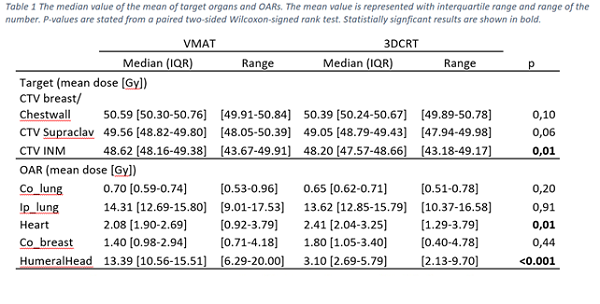
Similar
dose to OAR was achieved with VMAT compared to 3DCRT (Figure 1). Small
differences were observed in the mean dose to the heart and humeral head. The
heart dose was slightly reduced with VMAT, whereas the dose to the humeral head
was increased (Table 1). Target coverage
was similar, however, with a small statistically significant increase in coverage
of supraclavicular- and internal mammary nodes CTV’s (V45Gy) for VMAT.
Compared to 3DCRT, VMAT reduced the number of needed breath-holds during
treatment by 56 %. All the VMAT plans were measured with ArcCHECK and
clinically acceptable. Measurements had
a mean gamma pass rate (3 mm and 3 %) of 98.4 % with a range from 96.6 % to
99.8 %.
Conclusion
Auto-planning
of VMAT within the treatment planning system Pinnacle produced plans in a fast and
consistent manner requiring less interaction from the treatment planner, thus
potentially reducing inter-planer variations. The dose distribution of the
butterfly VMAT technique was similar to that for the conventional tangential
irradiation. The VMAT technique improved dose coverage of lymph nodes, without
increased dose to contralateral organs nor heart. Furthermore, the number of
breath-holds during treatment was reduced by a factor of two for the VMAT
treatments, thereby increasing patient comfort and reducing risk of patient
displacement. 1 shorturl.at/dsAGR