iCycle-Eclipse: a novel approach to automated multi-criterial treatment planning
Kristine Fjellanger,
Norway
PD-0748
Abstract
iCycle-Eclipse: a novel approach to automated multi-criterial treatment planning
Authors: Kristine Fjellanger1,2, Liv Bolstad Hysing1,2, Ben J. M. Heijmen3, Helge Egil Seime Pettersen1, Inger Marie Sandvik1, Turid Husevåg Sulen1, Sebastiaan Breedveld3, Linda Rossi3
1Haukeland University Hospital, Department of Oncology and Medical Physics, Bergen, Norway; 2University of Bergen, Institute of Physics and Technology, Bergen, Norway; 3Erasmus MC Cancer Institute, Department of Radiation Oncology, Rotterdam, The Netherlands
Show Affiliations
Hide Affiliations
Purpose or Objective
Automated treatment
planning can increase plan quality and consistency while sparing resources, and
has become a standard tool in many radiotherapy clinics. Erasmus-iCycle is a
well-known system for automated planning, producing Pareto-optimal dose
distributions according to a pre-defined wishlist.
Here we present a novel
approach, where iCycle dose distributions are translated into objective
templates for IMRT optimization in Eclipse. The method is validated on a set of
locally advanced non-small cell lung cancer (LA-NSCLC) patients, comparing the
deliverable iCycle-Eclipse (iC-E) plans to the manually created clinical plans
(CP).
Material and Methods
An iCycle wishlist for IMRT
of LA-NSCLC was developed and tuned according to clinical priorities. An oncologist and a treatment
planner were involved in this process. The order of priority for target and
OAR objectives was PTV, lungs, heart and esophagus. In addition, there were
hard constraints and objectives for normal tissue dose, and maximum dose
constraints for the spinal canal, brachial plexus and PTV.
The iCycle DVHs were
translated into patient-specific objective templates, with line objectives that
limit dose for all volume levels for each OAR, and imported into Eclipse.
Priorities and normal tissue objective settings were kept constant after tuning
based on a few patients. The templates were used for automated plan
optimization in Eclipse (no manual tuning), applying the same beam
configurations as for the clinical plans, resulting in the iC-E plans.
iC-E plans for 17 LA-NSCLC
patients were compared to the CP. All patients had a 6-beam, manually planned
IMRT CP in Eclipse. The prescribed dose was 60 or 66 Gy in 2 Gy fractions and dose
calculation was performed with Acuros XB 15.6. The Wilcoxon signed-rank test
(p<0.05) was used for statistical testing.
Results
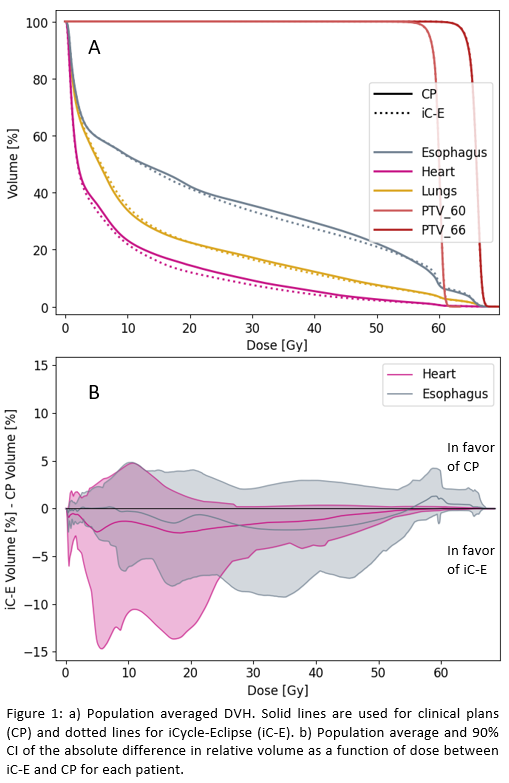
Target coverage and lung dose were similar between CP and iC-E, while
the average Dmean for heart and esophagus was significantly reduced
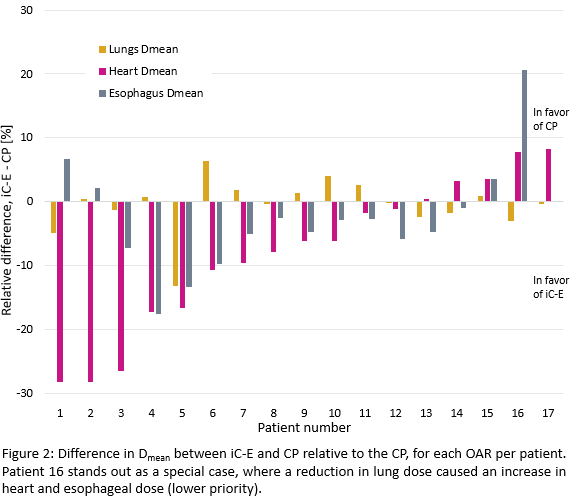
with iC-E [Fig. 1a, Table 1]. iC-E reduced heart Dmean for 12/17
patients and esophagus Dmean for 13/17 patients [Fig. 2]. For the
heart, it is noticeable that while the largest reductions with iC-E are for low
doses, there is also a consistent decrease in the medium-high dose range [Fig.
1b].
The maximum dose to the
spinal canal, brachial plexus and patient body followed the clinic’s
requirements for all plans.
Table 1: Comparison of
average dose metrics. Parameters in bold are significantly different.
Dose metric
| CP
| iC-E
|
PTV
V95% [%]
| 99.0
| 99.0
|
Lungs
Dmean [Gy]
| 13.4
| 13.4
|
Heart
Dmean [Gy]
| 8.5
| 7.7
|
Esophagus
Dmean [Gy]
| 22.9
| 22.3
|
Conclusion
The novel
iCycle-Eclipse method for automated treatment planning was developed and
validated on LA-NSCLC patients. A potential for sparing heart and esophagus dose
for most patients compared to manual plans was revealed. The new method allows
Eclipse to automatically generate plans that are close to Pareto-optimality.