We performed an
observational study using fieldwork and a structured observation.
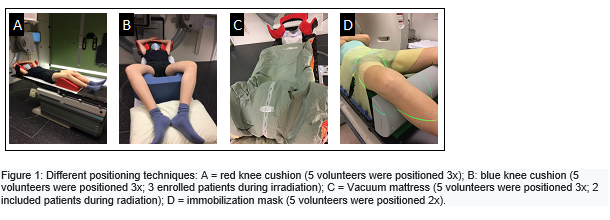
The used
positioning techniques are illustrated in figure 1. For frog-leg positioning a
blue knee cushion, a vacuum mattress and an immobilization mask (all ORFIT
industries) were used. For supine position, we used a red knee cushion (CIVCO
industries).
Five voluntary RTTs (mean age: 35y) underwent
all 4 positioning techniques. Five patients (mean age: 72y) being treated for
vulvar cancer were positioned using the blue knee cushion or the vacuum
mattress. Per individual positioning device, reproducibility, time (T) (rapid
positioning is indicative for the reproducibility and important for patient
comfort) and comfort was scored.
Reproducibility
was scored by the investigators using a score from 1 (very difficult) to 5 (very
easy)
T: was measured using 3 time-frames:
-T1: from the moment that the
patient/volunteer lies on the table until the moment of correct positioning.
-T2: on-line imaging and treatment.
-T3: time to get the patient/volunteer
from the treatment table.
Comfort was scored by the
volunteers/patients with numbers from 1 (no comfort) to 5 (very comfortable).